










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRSBO (Online)
versão On-line ISSN 1984-5685
RSBO (Online) vol.11 no.4 Joinville Out./Dez. 2014
ORIGINAL RESEARCH ARTICLE
Filling analysis of artificial lateral canals after main canal obturation through three different endodontic sealers
Tiago André Fontoura de Melo I; Denise Pereira Nunes I; Fernanda de Carvalho Modaffar Al-Alam I; Alexandre Azevedo Salles I; Renata Grazziotin Soares I
I Department of Dentistry, São Leopoldo Mandic Post-Graduation Center/SP – Porto Alegre – RS – Brazil
ABSTRACT
Introduction and Objective: This study aimed to evaluate, in vitro, the filling ability of lateral canals after main canal obturation through three different endodontic sealers. Material and methods: Thirty single-rooted pre-molars were used and, six lateral canals were constructed on proximal surfaces and arranged in pairs at 3, 5 and 7 mm from the apex. After chemo-mechanical preparation, with size #40 memory instrument, the teeth were randomly assigned to three experimental groups, according to the root canal sealer applied: Endofill® (group A), Sealer 26® (group B) and MTA Fillapex® (group C). In all groups, we used active lateral condensation technique with gutta-percha associated with sealer. After obturation, the teeth were radiographed at buccolingual direction and the images were digitized. The analysis of endodontic sealer plug near the lateral canals was performed by calculating the area through Image Tool® software. Results and Conclusion: The data were subjected to parametric (Anova), and nonparametric (Kruskal-Wallis) tests, with significance level of 5%. There was no difference among the tested sealers for filling the lateral canals. Concerning to the positions of lateral canals, no differences were also found among sealer types, except at 7 mm from the apex, where MTA Fillapex® showed a significantly greater filling than Sealer 26®.
Keywords: Endodontics; root canal obturation; runoff coefficient.
Introduction
Root canal system is anatomically complex with the presence of isthmuses, accessory and/or lateral canals, and apical delta which may either make difficult or prevent the proper cleaning and shaping, and consequently, the appropriate sealing of endodontic material 2.
The main goal of endodontic filling is the sealing of root canal system aiming at avoiding bacterial leakage. According to Siqueira Júnior et al. 14, the adequate sealing should prevent the percolation of peri-radicular exudates towards inside root canals and avoid possible bacterial reinfections.
To be considered as ideal, the endodontic sealer should exhibit some physical, chemical and biological qualities. Among these, the degree of sealer runoff is the capacity of penetrating inside the dentinal tubules and ramifications of the root canal system 13,21.
As far as we are concerned, and despite the constant improvement of the endodontic materials, dental market has not launched the ideal endodontic sealer with all desired qualities yet. According to Siqueira Júnior et al. 14 and Saleh et al. 12, an endodontic sealer having excellent antimicrobial action and optimum runoff can aid in the disinfection of root canal system.
Almeida et al. 1 evaluated different endodontic sealers (AH Plus®, Endométhasone®, Pulp Canal Sealer®, Sealapex®, Target H&D® and Sealer 26®) regarding to the runoff, filling and sealing of lateral canals artificially produced in human teeth. Through radiographic examination, they verified that none sealer was capable of completely filling the lateral canals.
On the other hand, Baisch et al. 2 analyzed the lateral canal filling through different filling techniques and observed that lateral condensation technique and Tagger's hybrid technique did not showed statistically significant differences in relation to the degree of filling of canals at apical third. Notwithstanding, at cervical and medium thirds, Tagger's hybrid technique showed the best results than those of lateral condensation.
According to the study of Raymundo et al. 9, lateral condensation technique is poorer than the use of McSpadden drill, Tagger's hybrid technique Thermafill® system, because there is the sealer runoff only to lateral canals.
Recently, Angelus® Company has launched into Brazilian dental market, a MTA-based endodontic sealer, so-called MTA Fillapex®, mainly because its excellent physical-chemical properties 5,17 and biocompatibility compared with those of the materials in the market 7.
According to the manufacturer, MTA Fillapex® is a paste-to-paste sealer composed of one paste containing MTA and other paste containing a disalicylate-based compound. By mixing the pastes, an ionic polymer is obtained. Although it seems that this material show optimum physical-chemical properties, further studies are still necessary to prove it.
Thus, this study aimed to evaluate the filling capacity of artificial lateral canals after main canal obturation with the following endodontic sealers: MTA Fillapex®, Sealer 26®, and Endofill®.
Material and methods
This study was approved by the Ethical Committee in Research of the institution. Thirty single-rooted pre-molars measuring from 20 to 22 mm were used. Their lengths were measured from the highest cusp to root vertex, with the aid of a digital caliper (Digimatic Caliper – Mitutoyo®, Illinois, USA).
Exclusion criteria comprised teeth with incomplete rhizogenesis, intra-radicular post and core, and endodontic treatment; presence of dental resorption, calcified root canals, dilacerations and root fractures. These were assessed through visual and radiographic examination.
Then, the teeth were randomly divided into three experimental groups (n=10), according to the endodontic sealer used: Endofill® (Dentsply/ Maillefer, Ballaigues, Switzerland), Sealer 26® (Dentsply/Maillefer, Ballaigues, Switzerland), and MTA Fillapex® (Angelus Indústria de Produtos Odontológicos S.A., Londrina, Paraná, Brazil).
Next, the working length was set at 1 mm shorter of root apex and the teeth were cleaned, shaped and filled by a single endodontist. Accordingly, the cervical third was prepared with the aid of La Axxess® bur (SybronEndo, Glendora, USA), size 20 taper.06, at 5 mm deep inside root canal.
To clean and shape the root canals, Flexo-File instruments, first and second series, (Dentsply/ Maillefer, Ballaigues, Switzerland) were employed, through step-back technique 20.
The number of use of each endodont ic instrument was standardized in five root canals. Memory instrument was set at size 40, by stepping back 1 mm from working length for size 45 instrument and 2 mm for size 50 instrument.
At every instrument change, the canals were irrigated with 2.5% sodium hypochlorite (Iodontosul – Industrial Odontológica do Sul Ltda., Porto Alegre, Brazil), and at the ending of the preparation the canals were irrigated with 17% EDTA (Iodontosul – Industrial Odontológica do Sul Ltda., Porto Alegre, Brazil) for 3 minutes, by stirring a size 40 instrument, followed by sodium hypochlorite irrigation to remove the smear layer produced by the root canal shaping.
To construct the lateral canals on the proximal surfaces (mesial and distal), a LN drill (Dentsply/Maillefer, Ballaigues, Switzerland), measuring 28 mm of length and 0.10 mm of diameter, coupled to a high-speed handpiece and a size 15 K type instrument (Dentsply/Maillefer, Ballaigues, Switzerland) were used up to communicate with the main canal of every teeth. Six lateral canals were constructed in pairs at 3, 5 and 7 mm from root apex, measured with the aid of a flexible plastic ruler (Faber-Castell, São Carlos, São Paulo, Brazil).
Before obturation, root canals were dried with absorbent paper points (Tanariman Indústria Ltda., Manaus, Amazonas, Brazil) of size matching the memory instrument (size 40) at working length.
Next, the main gutta-percha point (Tanariman Indústria Ltda., Manaus, Amazonas, Brazil) was selected so that it locked at the apical area of root canal at working length. After that, a radiograph was taken to prove the gutta-percha point locking.
The endodontic sealers were mixed according to the manufacturer's instructions on a glass plate (Preven Indústria e Comércio de Produtos Odontológicos, Paraná, Brasil), with the aid of a no. 24 spatula (SSWhite, Rio de Janeiro, Brazil). The ideal mixture should form a thread of approximately 2 cm, without disrupting, when the spatula was touched on and raised from the plate.
Following, the endodontic sealers were taken to root canals with the aid of the main gutta-percha point. Active lateral condensation technique was used. Size R7 accessory gutta-percha points (Tanariman Indústria Ltda., Manaus, Amazonas, Brazil), covered by the sealer, were also introduced into root canals with the aid of dental tweezers (SSWhite, Rio de Janeiro, Brazil) in the spaces obtained with the aid of a finger spreader (Dentsply/Maillefer, Ballaigues, Switzerland). Next, the points were cut with the aid of a heated Paiva plugger (SSWhite, Rio de Janeiro, Brazil), at the root canal entrance.
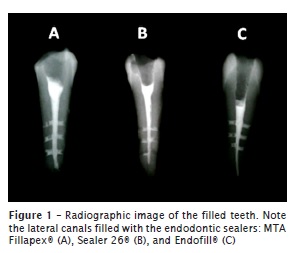
After obturation, a radiograph was standardly taken with the aid of a platform, so that the buccal surface always faced upwards (figure 1).
The paralleling radiograph technique was used with a 5 cm standardized distance between the x-ray cylinder and the radiographic film (ultra-speed DF-58, Eastman Kodak Company, Rochester, New York, USA). The x-ray device (TIMEX 70C – Gnatus Equipamentos Médico-Odontológicos Ltda., Ribeirão Preto, São Paulo, Brazil), was used with an exposure time of 0.8 seconds. Radiographic processing was carried out inside portable processing boxes by using developer solution (Eastman Kodak Company, Rochester, New York, USA) for 1 minute and fixer solution (Eastman Kodak Company, Rochester, New York, USA), for 10 minutes. Then, the radiographs were washed in running water for 20 minutes and let air dry.
Following, the radiographic images were digitized (LK-C41, Zhengzhou Linker Imp. & Exp. Co. Ltda., China). The analysis of the filling area of the endodontic sealer, in mm2, inside the lateral canals was determined through "area" tool from Image Tool® software (UTHSCA, San Antonio, TX, USA). The percentage of the filling area of the artificial lateral canal was calculated through rule of three. The obtained data were submitted to statistical analysis.
Results
Normal distribution was verified by applying Kolmogorov Smirnov test, with level of significance of 5%. Only the percentage of total filling had normal distribution. Accordingly, the parametric test (Anova) was applied to compare the total values. The nonparametric test (Kruskal-Wallis) was applied to compare the values of the lateral canals.
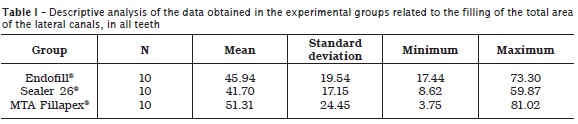
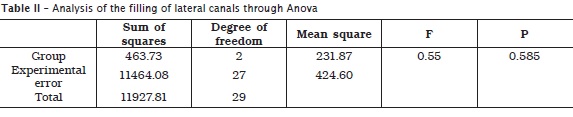
There were no statistically significant differences in the filling of the lateral canals among the three tested sealers (Anova, p = 0,585) (tables 1 and 2).
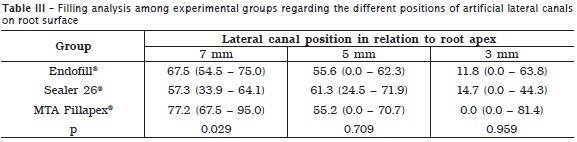
The analysis of the position of the artificial lateral canals through Kruskal-Wallis test showed no statistically significant differences among the experimental groups regarding to the percentage of filling, except at 7 mm from root apex, where MTA Fillapex® exhibited a significantly greater filling than that of Sealer 26® (table 3).
Discussion
Root canal sealing and filling quality by endodontic sealers is extreme relevant to evaluate and follow-up at long term both the endodontic treatment success and failure. The presence of not-filled lateral and accessory canals result in the maintenance of organic tissue, debris, and bacteria, as demonstrate by the study of Barkhordar and Stewart 3.
Accordingly, the aim of this study was to evaluate the filling capacity of MTA Fillapex®, by comparing it with that of Sealer 26® and Endofill®, during lateral canal obturation process. The rationale behind the choice of these sealers was their different physical-chemical and biological characteristics.
This study was conducted on extracted teeth because this methodology has been very employed to verify the influence of both the technique and endodontic sealer on the filling of the main canal ramifications 6,8.
The artificial lateral canals were obtained with the aid of a LN drill followed by a size 15 endodontic instrument, similarly to the studies of Goldberg et al. 6 and Zhang et al. 22. According to Venturi et al. 18, the diameter of the lateral canal reported in many studies is of 0.15 mm. In this present study, the lateral canals were made after the shaping of the main canal to avoid the smear layer formation, which could obliterate them.
Lateral condensation was used because it is the technique most used by endodontists and meets the study's objective, that is, to demonstrate the capacity of each endodontic sealer of filling artificial lateral canals. Many studies 4,9,10 have demonstrated that lateral condensation fills the main canal ramifications only with the sealer.
It could be observed by this present study that none endodontic sealer was capable of completely filling the artificial lateral canals. These results corroborate with those of the studies of Raymundo et al. 9, Almeida et al. 1, Tanomaru-Filho et al. 16, and Rebouças et al. 11.
The comparison among the three tested sealers did not exhibit any statistically difference regarding the filling of the lateral canal, in agreement with the study of Almeida et al. 1, who compared five different sealers: AH Plus®, Epiphany®, Endométhasone®, Pulp Canal Sealer® and Sealapex®.
In the analysis of the influence of the lateral canal location, the studies of Almeida et al. 1 and Souza et al. 15 also did not verify statistically significant differences. In the studies of Dulac et al. 4 and Venturi et al. 18, it was observed a greater root canal filling rate in the canal closest to the cervical third than in the canals at medium and apical thirds.
The apical area of root canal is the site of greatest prevalence of lateral canals. According to Villegas et al. 19, there is a prevalence of approximately 99% of accessory canals at the three apical millimeters, showing the complex anatomy, full of ramifications, of this area.
Conclusion
According to the results found, it can be concluded that there were no differences among the endodontic sealers tested regarding the filling of artificial lateral canals during obturation.
References
1. Almeida JF, Gomes BP, Ferraz CC, Souza-Filho FJ, Zaia AA. Filling of artificial lateral canals and microleakage and flow of five endodontic sealers. Int Endod J. 2007;40(9):692-9. [ Links ]
2. Baisch GS, Silveira LFM, Martos J. Análise radiográfica da repleção de canais secundários submetidos a duas técnicas de obturação. RPG Rev Pós-Grad. 2006;13(2):139-44.
3. Barkhordar RA, Stewart GG. The potential of periodontal pocket formation associated with untreated accessory root canals. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1990;70(6):769-72.
4. Dulac KA, Nielsen CJ, Tomazic TJ, Ferrillo PJJ, Hatton JF. Comparison of the obturation of lateral canals by six techniques. J Endod. 1999;25(5):376-80.
5. Faraoni G, Finger MS, Masson MC, Victorino FR. Avaliação comparativa do escoamento e tempo de presa do cimento MTA Fillapex®. RFO. 2013;18(2):180-4.
6. Goldberg F, Artaza LP, Silvio A. Effectiveness of different obturation techniques in the filling of simulated lateral canals. J Endod. 2001;27(5):362-4.
7. Gomes-Filho JE, Watanabe S, Bernabé PFE, Costa MTMA. Mineral trioxide aggregate sealer stimulated mineralization. J Endod. 2009;35(2):256-60.
8. Pécora JD, Ribeiro RG, Guerisoli DM, Barbizam JV, Marchesan MA. Influence of the spatulation of two zinc oxide-eugenol-based sealers on the obturation of lateral canals. Pesqui Odontol Bras. 2002;16(2):127-30.
9. Raymundo A, Portela CP, Leonardi DP, Baratto-Filho F. Análise radiográfica do preenchimento de canais laterais por quatro diferentes técnicas de obturação. RSBO. 2005;2(2):22-7.
10. Reader CM, Himel VT, Germain LP, Hoen MM. Effect of three obturation techniques on the filling of lateral canals and the main canal. J Endod. 1993;19(8):404-8.
11. Rebouças KS, Pithon MM, Neto MM. Avaliação radiográfica do preenchimento de canais laterais artificiais utilizando três técnicas de obturação. Rev Odontol Univ Cid São Paulo. 2013;25(2):126-34.
12. Saleh IM, Ruyter IE, Haapasalo M, Orstavik D. Survival of Enterococcus faecalis in infected dentinal tubules after root canal filling with different root canal sealers in vitro. Int Endod J. 2004;37(3):193-8.
13. Siqueira Júnior JF, Fraga RC, Garcia PF. Evaluation of sealing ability, pH and flow rate of three calcium hydroxidebased sealers. Endod Dent Traumatol. 1995;11(5):225-8.
14. Siqueira Júnior JF, Rocas IN, Favieri A, Abad EC, Castro AJ, Gahyva SM. Bacterial leakage in coronally unsealed root canals obturated with 3 different techniques. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2000;90(5):647-50.
15. Souza MA, Cecchin D, Farina AP, Menin MLF, Guisi AC, Barbizam JVB. In vitro evaluation of filling of lateral root canals with different filling materials by using digital radiography. Rev Odonto Ciênc. 2012;27(1):64-8.
16. Tanomaru-Filho M, Bosso R, Sant'Anna-Júnior A, Berbert FLCV, Guerreiro-Tanomaru JM. Effectiveness of gutta-percha and Resilon in filling lateral root canals using thermomechanical technique. Rev Odontol Unesp. 2013;42(1):37-41.
17. Torabinejad M, Watson TF, Pitt Ford TR. Sealing ability of mineral trioxide aggregate when used as a rood end filling material. J Endod. 1993;19(12):591-5.
18. Venturi M, Di Lenarda R, Prati C, Breschi L. An in vitro model to investigate filling of lateral canals. J Endod. 2005;31(12):877-81.
19. Villegas JC, Yoshioka T, Kobayashi C, Suda H. Obturation of accessory canals after four different final irrigation regimes. J Endod. 2002;28(7):534-6.
20. Walton RE. Histologic evaluation of different methods of enlarging the pulp canal space. J Endod. 1976;10(2):304-11.
21. Weis MV, Parashos P, Messer HH. Effect of obturation technique on sealer cement thickness and dentinal tubule penetration. Int Endod J. 2004;37(10):653-63.
22. Zhang C, Huang W, Sun Z, Hou B. A comparison of two gutta-percha master oints consisting of different phases in filling of artificial lateral canals and depressions in the apical region of root canals when using a warm vertical compaction technique. Int Endod J. 2011;44(11):1041-6.
 Corresponding author:
Corresponding author:
Tiago André Fontoura de Melo
Rua Eça de Queiróz, n. 466, apto. 701 – Petrópolis
CEP 90670-020 – Porto Alegre – RS – Brasil
E-mail: tafmelo@gmail.com
Received for publication: September 23, 2013
Accepted for publication: May 22, 2014
