










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRSBO (Online)
versão On-line ISSN 1984-5685
RSBO (Online) vol.11 no.4 Joinville Out./Dez. 2014
ORIGINAL RESEARCH ARTICLE
Access and use of secondary dental care of a large city of Rio Grande do Sul, Brazil
Caroline Schirmer I; Alex Elias Lamas II; Daniel Demétrio Faustino-Silva III
I Program of Integrated Health Residency, Conceição Hospital Group – Porto Alegre – RS – Brazil
II Oral Health Technic Area, Municipal Health Secretary – Porto Alegre – RS – Brazil
III Community health service, Conceição Hospital Group – Porto Alegre – RS – Brazil
ABSTRACT
Introduction: The Brazilian Dental Specialty Centers (CEOs) were created due to a limitation of Brazilian public dental care. In 2004, the specialized services corresponded to no more than 3.5% of total dental clinical procedures. These services are a reference for oral health teams in primary care in order to perform additional procedures at this level of attention. Despite the expansion of specialized procedures, the resolution of these services is subject to discussion between managers and researchers. Objective: To evaluate the access and use of the secondary dental care of a large city. Material and methods: The descriptive retrospective longitudinal study was conducted using CEO primary data from November 2012 to July 2013. These data were obtained from the Technical Department of Oral Health and the coordination of services were analyzed and then compared to the guidelines of Ordinance no. #1.464/MS. Results: The performance of services was low, ranging from 47.2 to 60.6% of the overall fulfillment of goals, in average. By analyzing per subgroup, endodontics was the subgroup with lower fulfillment (33.2%) and periodontics was that with the most fulfillment (88.3%). Absenteeism on the first appointments, the average per service ranged between 29.4 and 44.2%, and periodontics was the most affected subgroup (51%). The percentage of finished treatment ranged from 52.9 to 66.4%, and stomatology was the subgroup with less number of finished treatments (19.2%). Conclusion: The study revealed low utilization of the evaluated services associated with high absenteeism. Further studies and management initiatives are necessary to find ways to optimize secondary dental care integration to primary care services.
Keywords: health services evaluation; oral health care; health care networks.
Introduction
The Brazilian Unified Health System (SUS) was created by the Brazilian Federal Constitution from 1988 and proposes a model of health care towards promotion, protection, prevention and recovering of health, based on the doctrinal principles of universality, integrality and equity 3,13.
Within the context of SUS primary care, the Brazilian Primary Care Policy (PNAB) points out the necessity of the increasing of resolutivity of health services, and operationalization of integration among the many care levels 11,12. In the light of this, the Brazilian Oral Health Policy (PNSB), so-called Brasil Sorridente, is an important cornerstone to reorganize SUS dental care 7,12.
The Brazilian public dental care limitation is historical. It tends to prioritize mainly the primary care. The expansion of the secondary dental care did not follow the expansion of primary care and the large increasing of the population requirements.
It is perceived that the access of high-quality health services can alleviate unfavorable conditions of the population and interfere in the person's self-perception of oral health needs, so that they search the access to services 4. The evaluation of health services is important to define, based on the found results, optimization possibilities of these services inside the care network aiming to the comprehensive oral health care.
The Brazilian Dental Specialty Centers (CEOs) offer specialized oral health procedures and are secondary unities integrated to the regional planing that should minimally provide the following dental specialties: periodontics, endodontics, dental patients with special needs, oral diagnosis, and minor oral surgery. CEOs are classified into three types: type I (three dental chairs), type II (four to six dental chairs), and type III (more than seven dental chairs) 12.
CEOs funding is established by the Brazilian Ordinance no. 1.464/GM/MS, from 24 of June of 2011 10, and provided by the Brazilian Health Fund (FNS), which repass monthly values to the municipal health funds. This ordinance has an attachment comprising the minimum production per month, per specialty, to evaluate the performance. Type I CEO should inform SUS Information System and provide 80 individual preventive, basic operative dentistry, basic dental surgery procedures; 60 periodontal procedures; 35 endodontic procedures; and 80 oral surgery/oral and maxillofacial trauma procedures. Type II CEO should inform and provide 110 individual preventive, basic operative dentistry, basic dental surgery procedures; 90 periodontal procedures; 60 endodontic procedures; and 90 oral surgery/oral and maxillofacial trauma procedures. Type III CEO should inform and provide 190 individual preventive, basic operative dentistry, basic dental surgery procedures; 150 periodontal procedures; 95 endodontic procedures; and 170 oral surgery/oral and maxillofacial trauma procedures This Ordinance also states that to fullfill the minimum production per month, 50% of the basic procedures must be restorations and 20% of the endodontic procedures must be the obturation of a permanent teeth with three or more canals and/or retreatment cases.
Studies evaluating CEOs creation have discussed on the costs and found that they are very close to that of primary care and basically comprises staff payament with low performance of the services. A study development in the state of Pernambuco pointed out that only 40.9% of the CEOs fullfilled the goals with good performance in ambulatory production proposed by the central, inductor and formulator of the policy 5.
Additionally to the production analysis, one should investigate the structure, localization, performance, and CEOs creation characteristics. Medeiros 9 evaluated the structure of three CEOs in the city of Natal and observed problems related to the environment (dental offices of inadequate size and privacy), cleaning (leaks, musty walls, strong odors), the dental offices that comprised many specialties, but not exclusively for that use, the total working hours were not fullfilled, and the absence of instruments (mainly periodontal ones).
Chaves et al. 4 conducted a qualitative and quantitative study aiming to evaluate the offer and use of secondary dental care of four CEOs of the state of Bahia. They analyzed the potential production capacity proposed by the Ordinance GM/MS no. 1.101/2002 (three procedures per hour), the number of procedures calculated by experts through consensus technique (1.2 to 1.5 procedures per hour, depending on the specialty) and number of procedures calculated according to the standards proposed for CEOs habilitation (Ordinance GM/MS no. 1.571/2004, now replaced by Ordinance no. 1.464/2011). The study revealed that the use rates ranged according to the standard used, with values above 100% considering the standard proposed by the specific ordinance for CEO production standardization prevailing at that time and very low according to the standard proposed by the Ordinance GM/MS no. 1.101/2002. The use rates of the procedures according to the standard proposed by the experts ranged according to both the specialty and CEO, but generally demonstrated low use rates 4.
Guimarães 7 studied the oral health secondary care in the state of Ceará. Sixty-seven CEOs were identified, of which 45 were analyzed under PNSB guidelines. Only 37% reached either good or optimum performance, while 63% had either poor or regular performance. Basic procedure goals were fullfilled by 86.7% of CEOs, but less than half of this percentage (42.2%) reached the minimum goals for endotontic, periodontal and minor oral surgery specialties 7.
Goes et al. 6 evaluated Brazilian oral health secondary care in 613 CEOs. Of these, only 14.5% were located at South region. The performance assessment comprised the fulfillment of the goals established by the Ordinance GM/MS no. 1.464 and by measuring the Global Goal Fulfillment, according to the macroregion. Concerning to the procedures, 80% of the goals were fulfilled for basic procedures, 50% for periodontal and endodontic procedures and 26% for minor oral surgery procedures. When secondary care was evaluated per region, it was observed that 14.2% of CEOs had very poor performance (fulfillment of goal by only one specialty); of these, 22.5% were found in south macroregion, the greatest percentage. The services with optimum performance (fulfillment of goal by all specialties) were 18.8%; of these, only 12.4% were found in south macroregion, the smallest percentage 6.
A large unmet demand of oral health secondary care is observed, which makes unfeasible reaching one of the important APS guidelines, that is, care integrality. At the same time that many patients wait for dental appointments, the services have low vacancies and high absenteeism rates 2,8.
Despite of CEOs expansion, few studies have been conducted on oral health secondary care, particularly in the South area of Brazil. From a municipal management point of view, it is important to evaluate the access dimensions and the CEOs secondary care resolutivity.
This study aimed to evaluate the access and use of CEOs in a large city describing the current context of oral health secondary care. The main used indicators were the percentage of finished treatment and absenteeism per service and per specialty to verify CEOs performance inside the health network.
Material and methods
This descriptive observational longitudinal study was conducted with the coordination of the technic area of the municipal Health Secretary of a large city from the South Region of Brazil. This study was submitted and approved by the Ethical Committee in Research of both the institutional and the city.
Data collection was performed under the coordination of both the technic area and evaluated services. The primary data of the Ambulatory Production Report (APR) in the period from November 2012 to July 2013 from all installed CEOs. To participate in the study, the CEOs must be registered in the Brazilian Ministry of Health and presented production during the study period. All CEOs that did not provide APR were excluded from the study.
Descriptive analysis comprised the collection of data on the relationship between primary and secondary care, oral health teams per CEO, number of hours per specialty, number of professionals, physical structure, and location of each CEO.
Primary data from APR were collected from the three CEOS of the city, from the especialies of endodontics, periodontics, minor oral surgey, dental patients with special needs, and stomatology, composed of: number of first appointments per specialty; number of following appointments; end of treatment; and absenteism. Also, the number of CEO appointment availble for primary care was collected.
Both the indicators "absence to first appointments" and "treatment resolutivity" were calculated, respectively, by the average ratio of the number of absence to first divided bt the average of the number of available appointments, multiplied by 100; and the average ratio of the finished treatment per specialty divided by the average of the available first appointments multiplied by 100.
The performance assessment of the services was verified by the indicator "Global Goal Fulfillment". This indicator was calculate by the ratio obtained by dividing the average number of procedures of each specialty per month by the number of procedures of the goal of each specialty multiplied per 100, according to the guidelines of the Ordinance MS no. 1.464, from 2011. The goal was considered as fulfilled when a percentege greater or equal than 100% of the ordinance goal was achieve for each specialty. The service performance were classified according to the following parameters: very poor (CEO did not fulfill any goal), poor (CEO fulfilled only one goal), regular (CEO fulfilled two goals), good (CEO fulfilled three goals), and optimum (CEO fulfilled all goals) 6.
Results
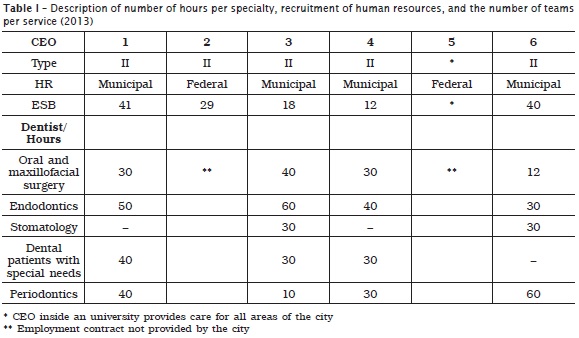
The communication between primary and secondary health care is achieved through referral and counter-referral system, with the aid of a form available in all oral health public services, in Brazil. The evaluated city have 45 oral health teams linked to the Brazilian family health programme (ESF), covering 10.96% in the year of 2013. Oral health care is also provided in the primary care units, under a different strategy: without linking with the region and community, resulting in referral to the secondary care. Oral health secondary care is provided by CEOs, composed of the five dental specialties required by the Brazilian Ministry of Health. One service also included the specialties of Dental Prosthesis and Temporomandibular Disorder (TMD). The number of hours per specialty, recruitment of human resources, and the number of teams per service are seen in table 1. During the analysis of data, in June 2013, a sixth CEO was created.
The secondary care apppointments is scheduled by ESB of the health care units by e-mail in five CEO and by the Scheduling Center in one CEO. Since the cases referred to secondary care were not classified, there was not priorities. The regulation is performed by the health care units, which are responsible for define the way they organized the patients's demands, either by waiting time or priority.
According to the Ordinance no. 599/GM/MS, all CEOs had at least four dental chairs, four or more dentists, totalizing at least 160 h of human resources. The recommendation of having one dental assistant per dental office was not followed by none of the CEOs.
To evaluate the ambulatory production, three CEOs participated in the study. Exclusion criteria comprised the creation date prior to the begining of the study and the absence of APRs during the collection of data.
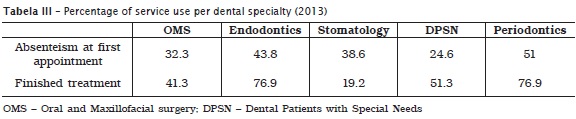
The absence at the first appoint per service ranged from 29 to 44% (table 2). By analysing each dental specialty individually, absenteism was even greater (table 3): dental patients with special needs exhibited the smaller percentage of missing appointments (24%), while periodontics showed the greatest percentage (51%).
The percentage of finished treatment was smaller in CEO B (52.9%). By analyzing per dental specialty, stomatology presented the smallest percentage (19,.%), while endodontics and periodontics showed the greatest percentages (77%).

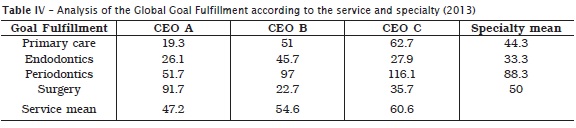
The performance assessment, through measuring the Global Goal Fulfillment showed that the performance of two CEOs was very poor and of one CEO was poor. Table 4 displays the percentage of each goal fulfillment, per dental specialty. Only the goal of periodontics was fulfilled with 116.1%. CEO C had the greatest fulfillment mean (60%). Moreover, the periodontal procedures had the greatest rate of fulfillment (88%) and endodontic procedured the smallest (33%), evidenced a discrepancy when the specialties were analyzed individually.
Discussion
CEOs can be examples of services providing oral health secondary and tertiary care through early diagnosis and immediate treatment, limitation of the damage, and rehabiliation, resulting in better oral health conditions 6.
Many factors influenced the access to the first appointment in secondary care. Within this context, municipal guidelines instructing and guiding dental practice of both levels are mandatory to qualify this process. The studied health care service, for many years, did not experienced expansion. The increasing of ESB teams and dentists in public health was timid until 2011. As of this year, the oral health resources were changed, resulting in the expansion of the population treated. The studied CEOs were created between 2004 and 2006, but with few dentists per specialty from the begining, making difficult to provide adequate care. Other problem is the waiting list 1,2; some specialties had a waiting time longer than one year for the appointment. Oral health care network is not managed through an electronic and unified database for scheduling the appointments, so that, each health care unit managed your own waiting list. According to Zaitter et al. 14, "one cannot search proper solutions for the waiting list without knowing the adequate lenght to know the real problem and propose solutions".
The absenteism rate was high, but this result is in agreement with other studies: Machado 8 found 32.9% and Bender et al. 2 found 34.4% of missing appointments. This latter study evaluated the absenteism in medical appointments, which proved that the problem is not restricted to oral health. Secondary care demonstrated serious contradictions because high indexes of requirements are observed, simultaneously to a severe number of missing appointments, resulting in idleness and burdening the system. The decrease in absenteism could cause a positive impact on the goal fulfillment and optimization of oral health secondary care.
The mean percentage of finished treatment per first appointment was low. At every ten patients, only five concluded the treatment at one studied service. Some factors can explain this results: problems with transportation, lack of patient's compliance, impossibility of missing workday, poor treatment provided by secondary, wrong referral by primary care and lack communication between the care levels. Futher studies on the causes of low treatment compliance are necessary so that the services become more resolutive.
To evaluate oral health secondary care, we used the Global Goal Fulfillment. This study found a low fulfillment of goals in all evaluated CEOs. Many causes can explaing these findings. Most of the studied CEOs had only one dentis per specialty. Moreover, few dentists were specialists in the area of expertise. The missing workday of the dentist by many reasons, but without repositon, directly reflects in the ambulatory production. It is necessary a policy on recruitment of human resources by the city. The dentist working in the studied CEOs came from primary care and were distributed by their area of interest of professional experience, without specialization if the area of expertise and without higher wages.
APR use as instrument for data collection can be described as this study's bias because the data were provided by the service coordinators based on the forms filled by the dentists. Accordingly, this may interfere in recording the information. Two CEOs were not evaluated because they did not fill the APR. One CEO is located inside a hospital with its own information system. The other CEO is located inside an university because it did not provide a production per month at the nine month period of this study. A standardized and unified guideline on the register of the information is necessary, regardless of the service, either public or private.
Conclusion
To understand the context of CEOs inside the health care network is important to understand the current challenges for the implantation. Both the qualification and organization of secondary care inside the network requires constant evaluation of absenteism and case resolutivity. The presence of an effective regulation system, protocols among services, large technic capacity, constant monitoring process, negotiation of goals, and discussion on working processes should be tools studied and used. The effective communication between primary and secondary care should be potentialized so that the patient is not punished because of difficulties existing at the two levels. The simple expansion of services do not assure they quality and resolutivity. Constant observation, negotiation and communication of secondary care processess and objectives are necessary to achieve greater transparency, effectiveness, and integration to health care network.
References
1. Awartani F. Broken appointment behaviour in a dental school environment. J Contemp Dent Pract. 2003 Nov;4(4):100-7. [ Links ]
2. Bender AS, Molina LR, Mello ALS. Absenteísmo na atenção secundária e suas implicações na atenção básica. Revista Espaço para a Saúde. 2010 Jun;11(2):56-65.
3. Brasil. Ministério da Saúde. O SUS de A a Z: garantindo saúde nos municípios/ Ministério da Saúde, Conselho Nacional das Secretarias Municipais de Saúde. 3. ed. Brasília: Editora do Ministério da Saúde; 2009.
4. Chaves SCL, Cruz DN, Barros SG, Figueiredo AL. Avaliação da oferta e utilização de especialidades odontológicas em serviços públicos de atenção secundária na Bahia, Brasil. Cad Saúde Públ. 2011 Jan;27(1):143-54.
5. Figueiredo N, Goes PSA. Construção da atenção secundária em saúde bucal: um estudo sobre os Centros de Especialidades Odontológicas em Pernambuco, Brasil. Cad Saúde Públ. 2009 Fev;25(2):259-67.
6. Goes PSA, Figueiredo N, Neves JC, Silviera FMM, Costa JFR, Pucca G et al. Avaliação da atenção secundária em saúde bucal: uma investigação nos centros de especialidades do Brasil. Cad Saúde Públ. 2012 Jul;28(Suppl.):S81-9.
7. Guimarães MLF. Cuidados secundários em saúde bucal: Centro de Especialidades Odontológicas no Ceará, Brasil, 2008. Fortaleza. Dissertação [Mestrado acadêmico em Saúde Pública]. Universidade Estadual do Ceará; 2010. 117 p.
8. Machado AT. Não comparecimento às consultas odontológicas na atenção secundária em município mineiro de grande porte. Dissertação [Mestrado]. Universidade Federal de Minas Gerais; 2013.
9. Medeiros E. Os Centros de Especialidades Odontológicas como suporte da atenção básica: uma avaliação na perspectiva da integralidade. Dissertação [Mestrado em Odontologia]. Universidade Federal do Rio Grande do Norte; 2007. 173 p.
10. Ministério da Saúde. Portaria n. 1.464/GM, de 24 de junho de 2011 [cited 2012 Oct 12]. Available from: URL:http://www.brasilsus.com.br/legislacoes/gm/108550-1464.html.
11. Ministério da Saúde. Secretaria de Atenção à Saúde. Departamento de Atenção Básica. Saúde bucal. Brasília: Ministério da Saúde; 2006.
12. Ministério da Saúde. Secretaria de Atenção à Saúde. Departamento de Atenção Básica. Política Nacional de Atenção Básica. 4. ed. Brasília: Ministério da Saúde; 2007.
13. Oliveira DC, Gomes AMT, Acioli S, Sá CP. O Sistema Único de Saúde na cartografia mental de profissionais de saúde. Texto Contexto – Enfermagem. 2007 Sep;16(3).
14. Zaitter WM, Silva M, Biazevic MGH, Crosato E, Pizzato E, Michel-Crosato E. Evaluation of patient access to medical specialty of Endodontics intwo health units in the city of Curitiba (PR). RSBO. 2009 Dec;6(4):414-21.
 Corresponding author:
Corresponding author:
Caroline Schirmer
Rua 7114, n. 23 – Restinga
CEP 91790-435 – Porto Alegre – RS – Brasil
E-mail: carolineschirmer@yahoo.com.br
Received for publication: July 16, 2014
Accepted for publication: August 12, 2014
