










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRSBO (Online)
versão On-line ISSN 1984-5685
RSBO (Online) vol.11 no.4 Joinville Out./Dez. 2014
Case Report Article
Endodontic surgery with simultaneous root canal filling: case report
Fernando Accorsi Orosco I; Lúcia Coelho Garcia Pereira I; Monica Misaé Endo I; Ralph Angeli Rangel I; Alexandre Silva Bramante II; Clóvis Monteiro Bramante II
I School of Dentistry, University Center of Anápolis – Anápolis – GO – Brazil
II Department of Operative Dentistry, Endodontics and Dental Materials, School of Dentistry of Bauru, University of São Paulo – Bauru – SP – Brazil
ABSTRACT
Introduction: Endodontic surgery is an excellent alternative for solving problems unsolved by conventional treatments and/or root canal retreatment. Objective: This study aims to report a clinical case of an endodontic surgery with simultaneous root canal filling. Case report: The left mandibular lateral incisor (#32) showed constant exudation even after root canal instrumentation and many changes of calcium hydroxide paste as intracanal medication. So, the treatment´s option was the endodontic surgery with simultaneous root canal filling for removing the periapical lesion. After the root canal filling, the curettage and apical plasty were made and the bone cavity was filled with calcium sulfate. Histopathological examination pointed out a periapical cyst. Conclusion: Endodontic surgery with simultaneous root canal filling of the tooth #32 was successful, once the patient did not exhibited any clinical symptoms, the exudate disappeared, and radiographically, it can be observed the formation of bone repair. The time of follow-up was of four months.
Keywords: Endodontics; surgery; root canal filling.
Introduction
The treatment indicated for endodont ic lesions with or without involving the apex is root canal treatment. When facing failure, endodontic retreatment is the option of choice, but not even this is a viable approach 8,11.
Endodontic surgery is an excellent alternative for solving problems unsolved by conventional treatment and/or retreatment of root canals and it is indicated in cases of maintenance of chronic periapical inflammation, with large radiolucent apical, restrict crown accesses up to root apex, post and core that cannot be removed, perforation, fracture of apical third, and impossibility of root canal filling due to constant exudation 2,10.
Among the surgical approaches most used in Endodontics, it can be cited: curettage with apical planning or apical plasty; apicoectomy, apicoectomy with retrograde obturation; and endodontic surgery with simultaneous root canal filling 1,2,8,17.
Endodontic surgery with simultaneous root canal filling aims to solve cases in which large chronic apical lesions with presence of persistent inflammatory exudate are maintained even after the good root canal shaping, many changes of calcium hydroxide intracanal medication, and with adjuvant antibiotics therapy, hindering the case conclusion 3,20.
Kuga et al. 10 emphasized that endodontic surgery with simultaneous root canal filling has as main advantage the obtainment of optimum apical sealing, once the exposed apex makes easy the direct visualization of gutta-percha point adaptation, in addition to a single-appointment treatment which simplifies the phases of conventional endodontic therapy.
This technique contraindications are the impossibility of previous debridement, presence of acute inflammation and inaccessibility to root apex 3,10,11.
Thus, this study aimed to report a clinical case in which endodontic surgery was executed with simultaneous root canal filling to demonstrate both the technique and operative steps and treatment success.
Case report
A Caucasian female patient, aged 53 years, was referred to the Dental Clinics of the institution (UniEvangélica). An endodontic treatment of tooth #32 had been performed for the last 6 months, comprising root canal shaping with apical stop constructed with the aid of size #30 file and 12 changes of intracanal medication composed of calcium hydroxide + distilled water paste (at every 15 days). Notwithstanding, root canal filling was not possible because of the exudate presence. In the light of this, endodontic surgery with simultaneous obturation of root canal was chosen.
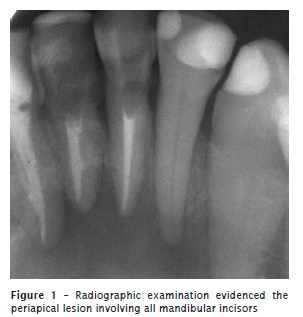
At clinical examination, patient reported sensitivity to palpation. Radiographic examination showed a large radiolucent area involving all four mandibular incisors (figure 1).
One hour prior to surger y, the pat ient took amoxicillin 875 mg (Aché Laboratórios Farmacêuticos, Guarulhos, São Paulo, Brazil). Antibiotics prophylaxis was performed because the root canal still presented persistent exudation indicating the high content of microorganisms.
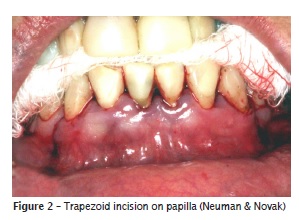
The patient was submitted to local anesthesia of the inferior alveolar nerve complemented by infiltrative anesthesia of the area with articaine hydrochloride 4% with epinephrine 1:100,000 (Articaíne, DFL Indústria e Comércio, Rio de Janeiro, Brazil). A trapezoid incision was performed on the papilla (Neuman & Novak) with the aid of no. #15 C scalpel blade (Embramac, Itajaí, Santa Catarina, Brazil), from left to right mandibular canine (figure 2).
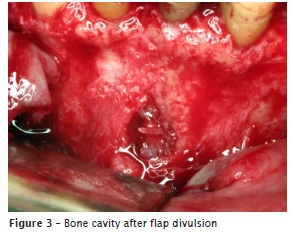
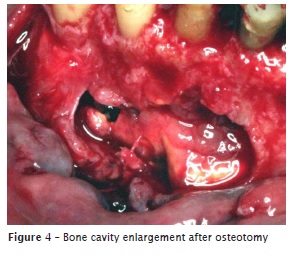
The flap divulsion evidenced a small bone cavity that was enlarged through osteotomy with the aid of Weldstaed, Mini Ochsebein and Ochsebein chisels (figures 3 and 4).
After bone osteotomy, the periapical lesion was clearly evidenced and was carefully removed with the aid of no. #11.5 dentin curette (Golgran Indústria e Comércio de Instrumentos Odontológicos Ltda., São Paulo, Brazil) and no. #5/6 Gracey curette (Golgran Indústria e Comércio de Instrumentos Odontológicos Ltda., São Paulo, Brazil). The lesion was completely removed and sent to histopathological analysis which pointed out an apical periodontal cyst (figure 5).

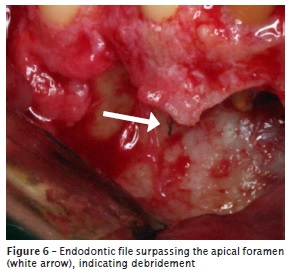
After the cleaning of bone cavity, root canal treatment was initiated by executing apical foramen debridement with size #15, #20 and #25 files aiming at promoting the cleaning of all root canal length (figure 6).
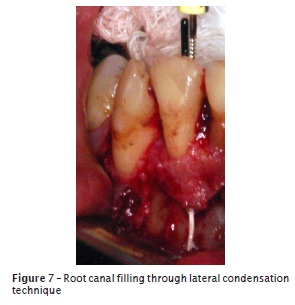
Root canal was again shaped, and apical stop was constructed with the aid of size #40 file and progressive step-backing up to size #55 file. Root canal filling was performed with the aid of gutta-percha points and endodontic sealer Endofill (Dentsply Indústria e Comércio Ltda., Petrópolis, Rio de Janeiro, Brazil), through lateral condensation (figure 7).
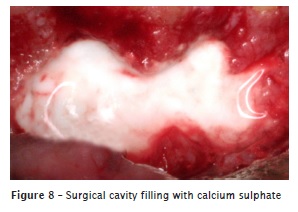
Following, gutta-percha points were cut and apically condensed with the aid of Paiva's plugger so that the filling material was contained only inside root canal, at 1.0 mm shorter of radiographic apex, which is the ideal position for root filling end. Also, we performed the apical plasty of all teeth exposed during surgery with the aid of an Bramante's apical file. To fill the surgical cavity, calcium sulphate + saline solution was used (Laboratório Farmacêutico Arboreto, Juiz de Fora, Minas Gerais, Brazil).
Simple suture points were performed and next, surgical cement was used to protect the suture.
Nimesulide 100 mg (Aché Laboratórios Farmacêuticos, Guarulhos, São Paulo, Brazil) for three days and amoxicillin 500 mg (Aché Laboratórios Farmacêuticos, Guarulhos, São Paulo, Brasil) for seven days were prescribed. Suture was removed after seven days. Tooth crown was restored 15 days after surgery.
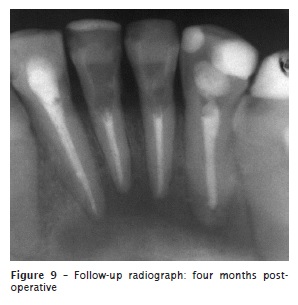
After 4 months, a follow-up radiograph was performed (figure 9). Both initial and follow-up radiographs were taken with the aid of radiographic positioner aiming at providing safeness and reliability to following-up procedure.
Discussion
Many authors 3,4,8,9,11 reported that endodontic surgery has very precise indications, that is, for cases in which endodontic treatment failed in solving problems in the apex and clinical symptomatology (pain and fistula) and bone rarefaction were still present.
The option for the trapezoid incision on the papilla (Neuman & Novak) is justified because of the large lesion and a triangular incision could make difficult to access and remove the lesion. According to Bramante and Berbert 4, a trapezoid incision on the papilla has the following advantages: excellent access to surgical field, visualization of all root length, and it is very difficult that this incision type is over the surgical cavity.
Flap divulsion was executed according to propose by Bramante and Berbert 4 and Leonardo and Leal 11, that is, it initiated at the junction of the horizontal and vertical incisions so that no damage was caused to the tissue and to enable the correct flap positioning during the suture procedure.
This present clinical case corroborates the affirmation of Kuga et al. 10 that the endodontic surgery with simultaneous root canal obturation is an important resource to be employed with indication for cases in which conventional endodontic treatment prognosis is doubtful, emphasizing the presence of persistent exudate. Moreover, this present clinical case is in agreement with the studies of Friedman 6 and Guimarães et al. 8, in which endodontic surgery should only be instituted after all possibilities of conventional endodontic treatment have been tried.
Still according to many authors 6,8,13,18, the surgical exposure of the apex makes easy root canal biomechanics; enables a more effective obturation through strong condensation without worrying about filling material extravasation; and the completely removal of the pathologic material from the apex results in a canal free of exudation, allowing the complete obturation and regeneration of the support tissue.
Among the materials employed for the filling of the surgical cavity, according to Pinto et al. 16, autogenous bone is the gold standard material because is composed of tissues of the own individual and it is the only material providing live immunocompatible bone cells, essential for phase I osteogenesis, accounting for the proliferation of bone cells, especially from the osteoid. Notwithstanding, autogenous bone graft is difficult to obtain, and other material types have been used, such as xenogenous grafts (e.g.: bovine bone matrix) and alloplastic grafts, as calcium sulphate. The rationale behind the filling of the surgical cavity with a solid paste of calcium sulphate + saline solution took into consideration the characteristics of this material: to be resorbable, biocompatible, osteoconductive; to stimulate bone neoformation; to be hemostatic; to act as a barrier in guided tissue regeneration against the formation of both conjunctive and epithelial tissue; to be of easy handling; and to decrease the surgical time 2,5,14-15,19.
Concerning to post-operative progress, Howe 9 stated that, generally, the patient should be followed-up at the first week after surgery and a periapical radiograph should be taken to evidence the periapical condition of the tooth at the immediate follow-up appointment. Radiographs at every three, six, 12 and 24 post-surgical months are important to determine the amount and speed of bone regeneration. In this present clinical case, the follow-up period was of 120 days (four months), at where the decreasing of the radiolucent area could be noted, evidenced the bone repair process.
Conclusion
Based on both the literature and the clinical case presented, it could be concluded that the endodontic surgery when well indicated and performed has a very favorable prognosis, because it eliminates the infection inside root canal, enabling root canal obturation, which consequently eliminates the infection in the periapical area, allowing bone neoformation.
References
1. Allgayer S, Bertoglio CRS. Remoção de núcleo intrarradicular seguida de obturação do canal radicular simultânea a cirurgia apical: oito anos de proservação. RFO Passo Fundo 2011 May/Aug;16(2):211-6. [ Links ]
2. Almeida-Filho J, Almeida GM, Marques EF, Bramante CM. Cirurgia paraendodôntica: relato de caso. Oral Sci. 2011 Jan/Dec;3(1):21-5.
3. Azambuja TWF, Bercini F, Alano F. Cirurgia paraendodôntica: revisão da literatura e apresentação de casos clínicos cirúrgicos. R Fac Odontol Porto Alegre. 2006 Apr;47(1):24-9.
4. Bramante CM, Berbert A. Cirurgia paraendodôntica. São Paulo: Santos; 2000.
5. Favieri A, Campos L, Burity V, Santa Cecília M, Abad EC. Use of biomaterials in periradicular surgery: a case report. J Endod. 2008 Apr;34(4):490-4.
6. Friedman S. Retrograde approaches in endodontic therapy. Endod Dent Traumatol. 1991;7:97-107.
7. Grung B, Molven O, Halse A. Periapical surgery in a Norwegian County Hospital: follow-up findings of 477 teeth. J Endod. 1990 Sep;16(9):411-7.
8. Guimarães KB, Post LK, Bezerra MF, Isolan CP, Hosni ES. Cirurgia parendodôntica com obturação simultânea dos canais radiculares: relato de caso clínico. R Ci Med Biol. 2006 May/Aug;5(2):188-94.
9. Howe GL. Cirurgia oral menor. 3 ed. São Paulo: Santos; 1990.
10. Kuga MC, Okamoto T, Brito JRO, Ribeiro Júnior PD, Tanaka H. Cirurgia paraendodôntica com obturação simultânea dos canais radiculares. Rev Assoc Paul Cir Dent. 1992 Jul/Aug;46(4):817-20.
11. Leonardo MR, Leal JM. Endodontia: tratamento de canais radiculares. 3. ed. São Paulo: Panamericana; 1998.
12. Lewis RD, Block RM. Management of endodontic failures. Oral Surg Oral Med Oral Pathol. 1988 Jun;66(6):711-21.
13. Molven O, Halse A, Grung B. Incomplete healing (scar tissue) after periapical surgery – radiographic findings 8 to 12 years after treatment. J Endod. 1996 May;22(5):264-8.
14. Pecora G, Andreana S, Margarone JE, Covani U, Sottosanti J. Bone regeneration with a calcium sulfate barrier. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1997 Oct;84(4):424-9.
15. Pecora G, De Leonardis D, Ibrahim N, Bovi M, Cornelini R. The use of calcium sulphate in the surgical treatment of a "through and through" periradicular lesion. Int Endod J. 2001 Apr;34(3):189-97.
16. Pinto JGS, Ciprandi MTO, Aguiar RC, Lima PVP, Hernandez PAG, Silva Júnior AN. Enxerto autógeno x biomateriais no tratamento de fraturas e deformidades faciais – uma revisão de conceitos atuais. Rev Facul Odontologia UPF. 2007;12(3):79-84.
17. Rossi RR, Sandri RN, Brunini SHS, Nascimento VR, Pfau EA, Tomazinho LF. Cirurgia parendodôntica para remoção de instrumento fraturado: relato de caso. Braz J Surg Clin Res. 2013/2014 Dec/Feb;5(1):51-4.
18. Rud J, Andreasen JO. Operative procedures in periapical surgery with contemporaneous root fillings. Int J Oral Surg. 1972;1:297-310.
19. Sellera DP, Mora OA, Murgel CAF, Godim Júnior E. Utilização clínica do enxerto de sulfato de cálcio na endodontia: técnicas e aplicações. Rev Assoc Paul Cir Dent. 2005 Mar/Apr; 59(2):137-43.
20. Sette-Dias AC, Maltos KLM, Aguiar EG. Tratamento endodôntico transcirúrgico: uma opção para casos especiais. Rev Cir Traumatol Buco-Maxilo-Fac. 2010 Apr/Jun;10(2):49-53.
 Corresponding author:
Corresponding author:
Fernando Accorsi Orosco
Centro Universitário de Anápolis, Curso de Odontologia
Avenida Universitária, km 3,5, bloco C, 4.o andar Cidade Universitária
CEP 75.083-515 – Anápolis – GO – Brasil
E-mail: fer_orosco@yahoo.com.br
Received for publication: September 26, 2013
Accepted for publication: May 15, 2014
