










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRSBO (Online)
versão On-line ISSN 1984-5685
RSBO (Online) vol.12 no.1 Joinville Jan./Mar. 2015
Original Research Article
Evaluation of elementary education teachers' knowledge on avulsion and tooth replantation
Simone Scandiuzzi FranciscoI; Adriana de Jesus SoaresII; Rodrigo Dutra MurrerI
I Dentistry Course, Leão Sampaio School – Juazeiro do Norte – CE – Brazil
II São Leopoldo Mandic School – Campinas – SP – Brazil
ABSTRACT
Introduction : Dental trauma care emergency is very important issue, especially in cases of avulsion and it is crucial for the prognosis. A preventive-educational approach had not been effective and there are many failures in handling dental trauma, mainly by lack of knowledge by health professionals, teachers and lay people. Objective: The aim of this study was to assess the knowledge of 89 teachers about dental trauma. Material and methods: A questionnaire divided into three parts containing questions about the emergency procedures in cases of dental trauma was applied. Results: Only 13% of teachers would replant the tooth in the socket, and only 7% said they would put the tooth in some liquid and 58% would store in a piece of paper, cloth or clean container. In relation to replantation, 75% reported that they would hold the tooth by the crown, 79% reported that first they would refer to the dentist, and 80% thought that the treatment had to be immediate. With regard to tooth preparation, 46% would keep it in saline, 24% in water, and only 11% in milk. Concerning to the avulsed tooth, only 15% correctly answered that they would replant the avulsed tooth and then referred to the dentist. Conclusion: It was concluded that the knowledge of teachers must be improved by educational and preventive campaigns on management of traumatized teeth.
Keywords: dental trauma; education health; dental avulsion.
Introduction
The Dentistry prioritizes the maintenance and integrity of teeth in the mouth, and the occurrence of dental trauma is difficult to reach this target, since its consequences involve functional, aesthetic, psychological, social and therapeutic damage, in addition to high costs for rehabilitation and monitoring for long periods of time 7,17,24.
In the presence of dental trauma, the oral structures are damaged on impact, which may cause changes in pulp and periodontal tissues, requiring an adequate emergency care and treatment. Treatment may be only the diagnosis of pulp and periodontal status, requiring palliative conduct to more complex treatments, in order to keep the tooth in a position to perform normal functions. The most common traumatic dental injuries are crown fractures involving enamel and enamel / dentine, but some injuries may be more serious, such as dental avulsion and intrusion, which require urgent immediate care as they could generate irreversible damage to the pulp and periapical tissues, leading to tooth loss 9.
Traumatic lesions such as crown fractures have a favorable prognosis for maintaining the vitality of the pulp compared with complicated crown fractures. The crown fracture not always develops pulp changes as obliteration of the canal or necrosis, however, when associated with tooth luxation, presents a significant deleterious effect on pulp prognosis, developing endodontic complications 7. On the other hand, the root fractures involve a combination of damage to the periodontal ligament, cementum, dentin, and pulp which are results from frontal impacts that force the tooth crown to the palatal region and the apical root portion labially. There is a more favorable prognosis when there is no compromise of the integrity of the pulp and periapical tissues, with the control of mobility and maintenance of pulp vitality of the fragments 9.
In periodontium, when low intensity impacts occur, small resorptions may develop whose prognosis is favorable because the newly formed cementum promotes repair. Most severe impacts results in luxations that cause periodontal ligament rupture, leading to tooth extrusion and even avulsion or intrusion by the impaction of the tooth in the socket.
Tooth luxation comprises the injuries that affect the periodontal ligament whose injury severity increases according to the tooth displacement after the impact. The lesions such as concussion and subluxation are those that cause no movement of the teeth, while the lateral luxation and extrusion, intrusion, and avulsion are those in which there is a large displacement of the tooth in the socket developing immediate or late complications, which favors the development of pulp necrosis and resorption 9.
Tooth avulsion is the complete removal of the tooth out of the socket and is considered a serious injury, which generates damage often irreversible with aesthetic and functional impairment, and may even lead to tooth loss, which directly affects the self-esteem and interpersonal relationship among people 1,6,14. The prevalence is 0.5% to 16%, involving children between 7 and 15 years of age, in whom the incidence is higher in upper central incisors 7. The treatment for avulsed teeth is the immediate dental replantation in an attempt to reinstate it to its original anatomical position, maintaining the function and integrity 8. Therefore, emergency care is crucial in trying to keep the tooth. Thus, the chances of replantation depend on an immediate response of the person injured in performing their own replantation or persons who are at the scene. And in cases where it is not possible to perform immediate replantation, management of injured teeth is equally important in order to maintain viable periodontal ligament fibers. In cases of tooth extraction, the shorter tooth staying out of the socket, the better the chances of success. The time from trauma to the tooth repositioning predisposes the development of complications, directly influencing the prognosis, making it unfavorable 7.
Currently, there is an increase of traumatic injuries among children and adolescents. Accidents occur mainly at home, on the streets and in schools, because of the type of play and the large number of activities and sports practices involving various modalities 7. For a good prognosis of traumatic injuries agility and knowledge about treatment are important, together with necessary information on the management of traumatic accidents for people who deal daily with children and adolescents, as well as to the lay population.
Studies on the knowledge of health professionals and teachers have demonstrated the lack of knowledge on the management of traumatic injuries in permanent and deciduous teeth 3,11,13,22-24,27,31,32,34. Thus, this study aims to verify the primary education teachers' knowledge working at private and public schools about the steps to be taken after the occurrence of dental trauma.
Material and methods
This study was submitted and approved by the Ethical Committee in Research of the UniEvangélica University Center (Anápolis – GO). The professors aged from 18 to 65 years were randomly evaluated and were willing in answering the questionnaire on the knowledge about the care after tooth trauma. A specific questionnaire was distributed for private and public primary schools.
The questionnaire was modified according to other studies in the literature 12,26,31, divided into three parts: part 1 verified the personal data of the professor; the part 2 dealt with the emergency care of tooth trauma, tooth avulsion experience; and what they would do facing tooth avulsion; part 3 assessed the professors' approach towards simulated tooth trauma situations. The answers were tabulated and presented as percentages.
Results
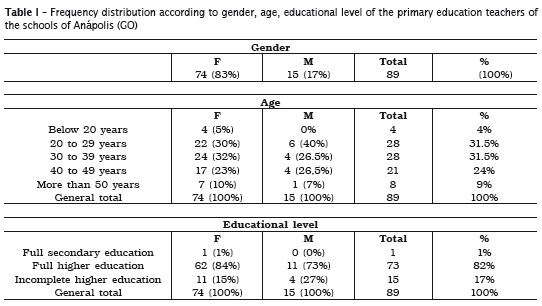
Eighty-nine professors participated in the study from private (46) and public (43) schools. All of them responded a questionnaire on tooth trauma. Part 1 comprised the personal and professional characteristics regarding age, gender, education level, professional experience, and instruction on first-aid care and tooth trauma (Table I). Part 2 was composed of basic questions on the importance of emergency situations, experience on tooth avulsion and which attitude toward the child experiencing tooth avulsion (Table II and III). Part 3 evaluated the knowledge through simulating clinical cases of tooth fracture and avulsion.
Most of the participants were female (83%), aged from 20-39 years (62%), with high education (84%), and professional expertise of 5-15 years (41%). About 47% of the professors received firstaid training, 98% were not instructed about tooth trauma, and 78% reported they did not know this subject. Of all professors, 96% would like to be instructed on tooth trauma (Table I).
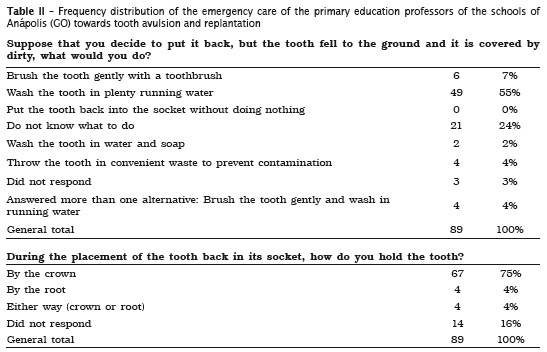
Part 2 demonstrated the lack of experience of the professor regarding to tooth trauma, because only 19% faced some case, and 79% would not replanted the avulsed tooth. Notwithstanding, if they had to replant, 75% would touch the tooth by the crown and 55% would wash the tooth in running water in case of dirty (Table II).
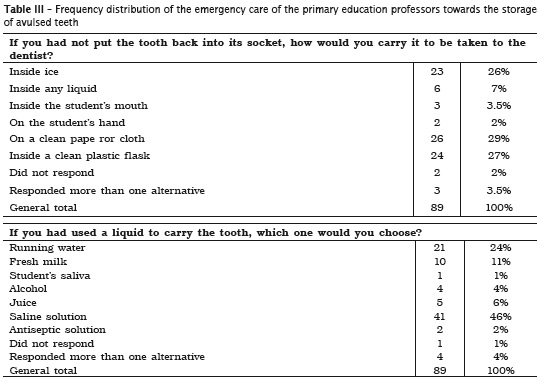
Concerning to the storage of the avulsed tooth, 58% of the professors would store it in dry environment, such as the student's hand, piece of paper or cloth, clean plastic flask; only 3% would place it inside the student's mouth and 7% would store it in wet environment. With regard the storage medium, 46% would use saline solution, 24% running water, and 11% milk (Table III).
Also, in case of tooth avulsion, 79% of the participants would refer the patient to a dentist and 80% considered that immediate treatment must be provided. Concerning to primary tooth, 52% reported that they knew how to differentiate a primary from permanent tooth, 16% indicated that the primary tooth should be replanted, and 47% did not know if the primary tooth should or should not be replanted. About 51% of the professors reported that they would search about tetanus vaccination, 37% reported that they would give medicaments to the child in case of pain after tooth trauma; of these, 82% would give analgesic drug, 12% anti-inflammatory drug, and 6% both analgesic and anti-inflammatory drugs.
Part 3 hypothetically simulated two tooth trauma situations to evaluate the attitude and knowledge of the professors, following the questionnaire of the clinical cases of tooth trauma. In case 1, we verified which the best attitude to be taken by the professors facing the following case: 9-year-old child fell down and hit the face, broking the front tooth, without injury and loss of consciousness. About 62% knew how to differentiate the maxillary permanent tooth involved in the case on enamel/ dentin fracture, 20% thought that the traumatized tooth was primary and 18% did not know how to answer. With regard to the immediate approach, 84 (94%) answered that first, they would call the parents and instruct to seek a dentist; of these only 42 answered that they would also search for pieces of the broken tooth.
In case 2, we verified which would be the best attitude of the professors towards the following case: 12-year-old girl fell from the stairs and injured the mouth with bleeding and tooth avulsion. Only 13 (15%) reported they would replant the tooth and send the child to the dentist immediately. About 61 (69%) professors answered that they would store the tooth in some liquid and refer the child to the dentist immediately.
Discussion
During the last decades, several studies have been published with worrying results regarding the lack of knowledge about dental trauma and management of traumatized teeth, both by lay people and health professionals 1-4,10,12,13,15,18-23,27,29,31,32,34,37,38. The results of this study confirmed the lack of knowledge about dental trauma in the training of elementary school teachers, similarly to international 2,12,25 and Brazilian 27,31,32studies. During the academic training of teachers, 47% had first aid training that not addressed the issue of dental trauma and 78% of teachers were unaware of it. This is worrisome because the school is considered an important and potentially favorable site to the occurrence of dental trauma for the children involved in physical activities and social 36. This result leads to the perception that the inclusion of this issue on first aid orientation during the pedagogical training of teachers is required.
Several factors also influence on the prognosis of avulsed teeth, such as trauma extension, extraalveolar time, handling and contamination of avulsed teeth, and storage medium 7. Tooth reimplantation success varies between 4% and 50%. This disparity is attributed to the conditions of the teeth and diversity of treatments. The literature recommends that avulsed teeth are immediately replanted because of the fragility of the periodontal ligament cells (PL) 7,16 . About 80% of the teachers answered correctly that the tooth should be replanted immediately and the dentist would be the first professional of choice, only 13% would replant the tooth. For measures to be taken in cases of tooth extraction, 24% of the respondents said they did not know what to do to help the child and 70% said they would not replanted the tooth. In this study there was a low rate of dental replantation, as in other studies in the literature 4,12. Although 75% of teachers answer correctly that the avulsed tooth should be handled by the crown and 55% respond that would wash in running water abundantly, few would realize the dental reimplantation.
A short extra-alveolar length time is best for the preservation of avulsed teeth, because of the development of the few areas of root resorption. In 1990, Andersson and Bodin 5 investigated human teeth replanted after 15 minutes and observed that most of the teeth had preserved its integrity and is recommended reimplantation as soon as possible. However, it is not always possible that the tooth is replanted just after avulsion, so that tooth must be properly stored 7.
The storage medium is a major factor influencing the prognosis of dental replantation because the tooth must be kept in a medium in which the pH, osmolarity and metabolism are physiologically compatible with the vitality of LP cells present on the root and in some cases even to stimulate its proliferation. The primary means of transport are: water, milk, physiological saline, Hank's balanced salt solution, ViaSpan and saliva.
Currently milk is considered one of the best storage medium because of their ideal physiological properties for maintaining the LP vitality for up to 6 hours, in addition to its easy access at the time of the accident, providing an adequate medium until searching for a dentist 7,8,27. In this study, for the storage, 58% of teachers would store the tooth on a piece of paper, clean cloth, clean plastic or hand of the student, that is, in a dry environment. In the case of transporting in liquid medium, only 11% knew that milk is the best storage medium, 46% would store in saline and 24% water. The lack of knowledge on the storage medium and dental replantation has been reported by previous studies 12,27,31.
Of the most frequent traumatic dental injuries, crown fractures involving enamel and enamel/ dentine are those that most affect young people 7,14. Evidence shows the negative impact of dental trauma among teenagers, because the smile's appearance plays an important role in the composition of facial aesthetics and the presence of traumatic injuries can hinder social interaction of individuals affected 14. The dental trauma involves several cosmetic changes, in addition to dental fracture it may result in color change of teeth, tooth mobility, pulp pathologies and pain. The restoration of a fractured tooth must have a satisfactory level in relation to aesthetics, because even in cases of simple fractures, there is need for appropriate follow-up, since the prognosis of crown fractures depends not only on an accurate diagnosis, but also on appropriate restorative procedures 30. The treatment of traumatic dental injuries is an important health promotion strategy that can significantly prevent negative biological and social impacts 19,33.
In the clinical case describing the crown fracture, about 62% of the teachers recognized that the incisor tooth is one of the permanent dentition in a 9 year-old child and 94% said they first come into contact with parents and would advise to look for the dentist; of these, 47% said they also seek the pieces of the broken tooth. Although most teachers consider important to refer to the dentist, is still low the number of teachers who seek the dental fragment, showing lack of proper care. Also in relation to the first case, 52% said they knew the difference between a primary from a permanent tooth. This is worrisome because the emergency treatment for primary teeth, especially in cases of avulsion, is not the replantation, to avoid compromising the development of permanent tooth 16.
In the case in which the child suffered tooth avulsion, only 15% reported that they would place the tooth back in its place and would take the child to the dentist immediately. The time between avulsion of the tooth and its replantation is considered of paramount importance for the prognosis of the avulsed tooth. Often lay people do not have proper evaluation of how critical this period is. Over time, the periodontal ligament cells adhered to tooth will necrotizing rapidly and success rate decreases vertically. Extra-alveolar periods longer than two hours almost always determine intense resorptions and therefore a poor prognosis 8.
In cases of avulsion, it is recommended prophylactic administration of tetanus vaccine and antibiotics because of tooth infection and also to prevent inflammatory resorption 7,9,16. In this study, 51.0% of teachers reported that they would investigate about the tetanus vaccination and 37% reported that they would give medications to the child in case of pain after suffering dental trauma, with the analgesic being the drug of choice, similar to other studies. Although the analgesic drug is beneficial in aiding the pain relief, the drug prescription by lay people should not be performed because of the possibility of occurrence of allergy or even drug interactions.
This study revealed that most teachers were not able to make the correct emergency care and did not receive adequate training on this. Whereas a favorable prognosis for avulsed / replanted depends significantly on the triad time the tooth remained outside the mouth, storage and appropriate transport medium, and minimal aggression to the root surface, knowledge of the emergency care of traumatic injuries is essential for tooth reestablishment and permanence in the mouth 19,29,32,35.
Lay people, such as teachers and parents, are usually present at the time of the accident and may be the first to provide initial care. Nevertheless, several studies show the unpreparedness of them to properly handle the situation 19,22,23,29.
According to Al-Asfour et al. 2, a lecture followed by discussion seems to be an efficient method to increase the knowledge and management of traumatic injuries. Following administration of a lecture, the authors found that there was an improvement of 39% to 97% in the general knowledge of avulsion. Given the above, it is highlighted the need for multidisciplinary interaction between health professionals (dentists, doctors, nurses) and teachers, who are information multipliers. So, there will be a positive interaction in health promotion and prevention of post-traumatic complications. Halawany et al. 19 found that well-qualified teachers are better able to make the right decisions in the management of emergencies related to tooth avulsion.
Mori et al. 26 obtained positive results after conducting an educational campaign, with leaflets, posters and lectures for health promotion and expansion of knowledge about dental trauma for professionals in schools. Thus, the use of clear and simple information is one of the best ways to improve the treatment success of avulsed permanent teeth and emergency management of traumatic injuries.
It is essential to implement public health policies that enable the reduction in the prevalence of traumatic dental injuries through legislation, prevention and education. More efforts are needed to expand the knowledge related to the promotion and maintenance of health, with parents, teachers and professionals the main people involved. One of the strategies for health promotion related to dental trauma is the expansion and recognition by health professionals and the general public that traumatic injuries can be prevented when associated with education campaign on dental trauma in schools and in the community. Health professionals can contribute in this sector through information and awareness of the importance of the use of mouthguards during sports and in treating dental trauma by correctly registering the place, time, cause, and human intention. Thus, we can identify acts of violence, whose information can contribute to the responsible agencies in the development of an individual protection efficient policy. The school environment is considered a suitable place to start an education program in oral health and dental trauma prevention , because more than one billion children are present in schools all over the world, in addition to teachers, school employees, students of parents and community involved. Programs of prevention and health promotion can strengthen, throughout the school life of children, basic health concepts to improve self-esteem, social behaviors, and life skills. In addition, these programs can humanize the school environment and implement policies and practices that offer multiple opportunities for health 28. Educational campaigns to prevent accidents involving dental trauma should be instituted in order to minimize the damage caused by traumatic injuries.
Conclusion
Based on the analysis of the data, it was concluded that there are many failures in the management of dental trauma, mainly by the lack of knowledge and, therefore, development of instruction programs for elementary school teachers and staff on emergency procedures in cases of trauma and tooth extraction should be consider.
References
1. Abu-Dawoud M, Al-Enezi B, Andersson L. Knowledge of emergency management of avulsed teeth among young physicians and dentists. Dent Traumatol. 2007;23(6):348-55. [ Links ]
2. Al-Asfour A, Andersson L, Al-Jame Q. School teachers' knowledge of tooth avulsion and dental first aid before and after receiving information about avulsed teeth and replantation. Dent Traumatol. 2008;24(1):43-9.
3. Al-Jundi SH. Knowledge of Jordanian mothers with regards to emergency management of dental trauma. Dent Traumatol. 2006;22(6):291-5.
4. Andersson L, Al-Asfour A, Al-Jame Q. Knowledge of first-aid measures of avulsion and replantation of teeth: an interview of 221 Kuwaiti schoolchildren. Dent Traumatol. 2006;22(2):57-65.
5. Andersson L, Bodin I. Avulsed human teeth replanted within 15 minutes – a long-term clinical follow-up study. Endod Dent Traumatol. 1990;6(1):37-42.
6. Andreasen JO. Luxation of permanent teeth due to trauma. A clinical and radiographic followup study of 189 injured teeth. Scand J Dent Res. 1970;78(3):273-86.
7. Andreasen JO, Andreasen FM. Textbook and color atlas of traumatic injuries to the teeth. 3. ed. Copenhagen: Mosby; 1994.
8. Andreasen JO, Borum MK, Jacobsen HL, Andreasen FM. Replantation of 400 avulsed permanent incisors. 4. Factors related to periodontal ligament healing. Endod Dent Traumatol. 1995;11(2):76-89.
9. Araujo M, Valera M. Injúrias por luxação. In: Araujo M, Valera M (eds.). Tratamento clínico dos tramatismos dentários. São Paulo: Artes Médicas; 1999. p. 189-205.
10. Blakytny C, Surbuts C, Thomas A, Hunter ML. Avulsed permanent incisors: knowledge and attitudes of primary school teachers with regard to emergency management. Int J Paediatr Dent. 2001;11(5):327-32.
11. Caglar E, Ferreira LP, Kargul B. Dental trauma management knowledge among a group of teachers in two south European cities. Dent Traumatol. 2005;21(5):258-62.
12. Chan AW, Wong TK, Cheung GS. Lay knowledge of physical education teachers about the emergency management of dental trauma in Hong Kong. Dent Traumatol. 2001;17(2):77-85.
13. Cohenca N, Forrest JL, Rotstein I. Knowledge of oral health professionals of treatment of avulsed teeth. Dent Traumatol. 2006;22(6):296-301.
14. Cortes MI, Marcenes W, Sheiham A. Impact of traumatic injuries to the permanent teeth on the oral health-related quality of life in 12-14-year-old children. Community Dent Oral Epidemiol. 2002; 30(3):193-8.
15. De Franca RI, Traebert J, De Lacerda JT. Brazilian dentists' knowledge regarding immediate treatment of traumatic dental injuries. Dent Traumatol. 2007;23(5):287-90.
16. Flores MT, Andersson L, Andreasen JO, Bakland LK, Malmgren B, Barnett F et al. Guidelines for the management of traumatic dental injuries. II. Avulsion of permanent teeth. Dent Traumatol. 2007;23(3):130-6.
17. Frujeri ML, Costa Jr ED. Effect of a single dental health education on the management of permanent avulsed teeth by different groups of professionals. Dent Traumatol. 2009;25(3):262-71.
18. Fujita Y, Shiono Y, Maki K. Knowledge of emergency management of avulsed tooth among Japanese dental students. BMC Oral Health. 2014;14(1):34.
19. Halawany HS, AlJazairy YH, Alhussainan NS, AlMaflehi N, Jacob V, Abraham NB. Knowledge about tooth avulsion and its management among dental assistants in Riyadh, Saudi Arabia. BMC Oral Health. 2014;14:46.
20. Hu LW, Prisco CR, Bombana AC. Knowledge of Brazilian general dentists and endodontists about the emergency management of dento-alveolar trauma. Dent Traumatol. 2006;22(3):113-7.
21. Jorge KO, Ramos-Jorge ML, de Toledo FF, Alves LC, Paiva SM, Zarzar PM. Knowledge of teachers and students in physical education's faculties regarding first-aid measures for tooth avulsion and replantation. Dent Traumatol. 2009;25(5):494-9.
22. Karande N, Shah P, Bhatia M, Lakade L, Arora MNABN, Bhalla M. Assessment of awareness amongst school teachers regarding prevention and emergency management of dentoalveolar traumatic injuries in school children in Pune City, before and 3 months after dental educational program. J Contemp Dent Pract. 2012;13(6):873-7.
23. Kaur H, Kaur S, Kaur H. Prehospital emergency management of avulsed permanent teeth: Knowledge and attitude of school teachers. Indian J Dent Res. 2012;23(4):556.
24. Losso EM, Tavares MCR, Bertoli FMP, Baratto- Filho F. Traumatismo dentoalveolar na dentição decídua. RSBO. 2011;8:e1-e20.
25. McIntyre JD, Lee JY, Trope M, Vann Jr WF. Elementary school staff knowledge about dental injuries. Dent Traumatol. 2008;24(3):289-98.
26. Mori GG, Castilho LR, Nunes DC, Turcio KH, Molina RO. Avulsion of permanent teeth: analysis of the efficacy of an informative campaign for professionals from elementary schools. J Appl Oral Sci. 2007;15(6):534-8.
27. Mori GG, Turcio KH, Borro VP, Mariusso AM. Evaluation of the knowledge of tooth avulsion of school professionals from Adamantina, Sao Paulo, Brazil. Dent Traumatol. 2007;23(1):2-5.
28. Moyses ST, Moyses SJ, Watt RG, Sheiham A. Associations between health promoting schools' policies and indicators of oral health in Brazil. Health Promot Int. 2003;18(3):209-18.
29. Murali K, Krishnan R, Kumar VS, Shanmugam S, Rajasundharam P. Knowledge, attitude, and perception of mothers towards emergency management of dental trauma in Salem district, Tamil Nadu: a questionnaire study. J Indian Soc Pedod Prev Dent. 2014;32(3):202-6.
30. Olsburgh S, Jacoby T, Krejci I. Crown fractures in the permanent dentition: pulpal and restorative considerations. Dent Traumatol. 2002;18(3):103-15.
31. Pacheco LF, Filho PF, Letra A, Menezes R, Villoria GE, Ferreira SM. Evaluation of the knowledge of the treatment of avulsions in elementary school teachers in Rio de Janeiro, Brazil. Dent Traumatol. 2003;19(2):76-8.
32. Panzarini SR, Pedrini D, Brandini DA, Poi WR, Santos MF, Correa JP et al. Physical education undergraduates and dental trauma knowledge. Dent Traumatol. 2005;21(6):324-8.
33. Ramos-Jorge ML, Peres MA, Traebert J, Ghisi CZ, de Paiva SM, Pordeus IA et al. Incidence of dental trauma among adolescents: a prospective cohort study. Dent Traumatol. 2008;24(2):159-63.
34. Sae-Lim V, Lim LP. Dental trauma management awareness of Singapore pre-school teachers. Dent Traumatol. 2001;17(2):71-6.
35. Santos ME, Habecost AP, Gomes FV, Weber JB, Oliveira MG. Parent and caretaker knowledge about avulsion of permanent teeth. Dent Traumatol. 2009;25(2):203-8.
36. Traebert J, Bittencourt DD, Peres KG, Peres MA, de Lacerda JT, Marcenes W. Aetiology and rates of treatment of traumatic dental injuries among 12-year-old school children in a town in southern Brazil. Dent Traumatol. 2006;22(4):173-8.
37. Traebert J, Traiano ML, Armenio R, Barbieri DB, de Lacerda JT, Marcenes W. Knowledge of lay people and dentists in emergency management of dental trauma. Dent Traumatol. 2009;25(3):277- 83.
38. Westphalen VP, Martins WD, Deonizio MD, da Silva Neto UX, da Cunha CB, Fariniuk LF. Knowledge of general practitioners dentists about the emergency management of dental avulsion in Curitiba, Brazil. Dent Traumatol. 2007;23(1):6-8.
 Corresponding author:
Corresponding author:
Simone Scandiuzzi Francisco
Rua João Francisco Sampaio, s/n, Cond. Terra dos Kariris, casa 1
CEP 63180-000 – Barbalha – CE – Brasil
E-mail: simonescan@gmail.com
Received for publication: February 28, 2014
Accepted for publication: September 2, 2014
