










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRSBO (Online)
versão On-line ISSN 1984-5685
RSBO (Online) vol.12 no.1 Joinville Jan./Mar. 2015
Original Research Article
Assessment of knowledge about oral cancer: study with students of public education
Iara Fiorentin ComunelloI; Elisabete Rabaldo BottanI; Constanza MarínI; Eduardo Mazzetti SubtilII
I Dentistry Course, University of Vale do Itajaí – Itajaí – SC – Brazil
II Medicine Course, University of Vale do Itajaí – Itajaí – SC – Brazil
ABSTRACT
Introduction and Objective: To evaluate the level of knowledge about oral cancer of students attending public school in one city of Santa Catarina (Brasil). Material and methods: A descriptive crosssectional study, using primary data collection. Students of last year of elementary school and first year of high school, enrolled in public schools in the city of Itajaí (SC), in 2012, were the target population. The non-probability sample was obtained by convenience. Data were collected through a self-administered questionnaire structured with 13 questions divided into three fields. The level of knowledge was made based on pre-established scores. Results: 1149 instruments were analyzed (80.8% of the target population). The average age of the group was 15.5 years and 54.5% were female. The majority (78%) never had received information about oral cancer. Only 27.9% had cognizance about self-examination of the oral cavity. With regard to knowledge, 87.5% classified as unsatisfactory. For most issues the cognitive field did not identify a significant correlation between knowledge and the variables gender and education. When asked if they would like to participate in educational and preventive activities about oral cancer and other issues related to health, 72.6% expressed interest. Conclusion: The group did not have adequate knowledge on the subject of oral cancer. Facing this reality, and the positive attitude of respondents, the researchers designed and offered an educational program to the research subjects.
Keywords: primary health care; oral neoplasm; disease prevention.
Introduction
Oral cancer, usually because of its treatment, can cause impairment in areas of the face, resulting in permanent dysfunction in essential activities for survival, such as feeding and socializing. This disease is considered a public health problem. In Brazil, it ranks the seventh place among all cancers diagnosed. To reverse this scenario, investment in public policies is necessary to support actions that lead to the reduction of morbidity and mortality for oral cancer1,3,19,24,25.
The Primary Health Care (PHC) based on educational measures, governed by the principles of health promotion, is considered essential to the improvement of health indicators and the population's quality of life. Therefore, with respect to oral cancer, the early diagnosis can create opportunities better life condition to people5,8,14.
The Declaration of Alma-Ata, synthesis document of the International Conference on Primary Health Care which took place in September 1978, already described minimum actions required to implement the primary health care to be developed in different countries. And among the actions, are those aimed at prevention and protection. Health education should be understood as a combination of opportunities that favor the maintenance and health promotion. Educational practices should be designed to target the subjects' autonomy in the conduct of their lives1.
Thus, among social spaces that enable the promotion of the educational process in health care, it is understood that the school is a fundamental place. Therefore, health education programs in schools should be encouraged, involving students, teachers, health workers, parents, dentists, and other health professionals.
This research was based such assumptions, because it aimed to evaluate the knowledge level of scholars from the public schools of Itajaí (SC, Brazil) on oral cancer.
Itajaí is a city of Santa Catarina (Brazil), located at the north central coast of Santa Catarina. It occupies a land area of 288 km2, with a population of 183,373 inhabitants, resulting in a population density of 636 inhabitants/km2. The Municipal Human Development Index in 2010 was 0.795. The territory space of the city is divided into 17 districts9.
According to data from the Brazilian Institute of Geography and Statistics9, in the city, in 2012, there were 12 public schools with high school, with a total enrollment of 6,092 students. And, there were ten public schools with basic education (5th to 9th grades), with 3,838 students. And among these schools, some offer both primary and secondary education.
The sociodemographic characteristics of Itajaí, together with its location (coastal region), justify the concern of the researchers on the prevention of oral cancer, so the results of this research are essential to the proposition of education-prevention activities aimed to these individual's profile.
Material and methods
The research is characterized as a descriptive, cross-sect ional study through primary data collection, which was conducted in Itajaí (SC, Brazil). The project was submitted and approved by the Ethics Committee in Research of Univali under protocol n. 171/11a.
To define the target population of the survey, only the students enrolled in 2012, at the last year of primary school and junior high first from 12 public schools located in nine districts were selected by raffle. According to records of the Department of Regional Development / Regional Education Management, the total number of enrolled students was 1,422.
To this target population, a non-probability sampling design was defined. The subjects were included in the study, since, after being informed about the research, they signed the Free and Clarified Consent Form (FCCF).
The instrument for data collection was a questionnaire with 13 open and closed type questions. The questions were divided into three fields. The first field, with three questions of the closed type, referred to the sociodemographic characteristics of the sample. In the second field were included five types of closed type on attitudes of respondents regarding the educational-preventive process in relation to oral cancer. The third field contained five questions of closed type involving specific knowledge on the subject of oral cancer.
The instrument of data collection was pre-tested in 2.5% (n = 36) of the target population through a pilot study in order to assess the applicability of the questionnaire and the adequacy of the questions. The pilot result denoted the need to reformulate two questions, which was performed. These questionnaires did not comprise the search.
Data collection was per formed by two researchers, by defined schedule in agreement with the schools. In each group, the researchers provided explanations on the project and then gave the FCCF to those interested in participating, to express their agreement by signing it. Students below 18 years, in addition to signing the FCCF, also had their parents sign the FCCF. Only after this ethical care, the questionnaire was delivered, which was answered in the classroom, anonymously.
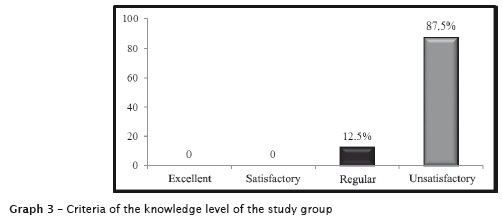
The assessment of the level of knowledge (field three of the questionnaire) was made based on the following scores: excellent – for a percentage of correct answers between 100% and 85%, satisfactory – for a percent of correct answers between 84% and 70%; regular – for a percentage of correct answers between 69% and 60%; and unsatisfactory – for a percentage of correct answers less than 60%.
Data were tabulated with the aid of Excel software for Windows and submitted to descriptive statistics. To assess the association between the level of knowledge of the students and the variables sex and education, nonparametric test (Chi-square) was applied, with level of significance set at lower than 0.01 (p < 0.01).
Results
1,149 questionnaires fully completed returned, representing 80.8% of the target population.
The female subjects percentage was 54.5% (n = 626) and 45.5% were males (n = 523). The age of respondents ranged from 13 to 37 years, with mean age of 15.5 years.
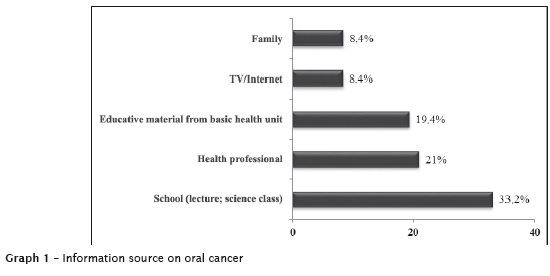
Most of the respondents (78%; n = 896) claimed never received information about oral cancer. Among those who had received some instruction (n = 253), the main sources mentioned were: school, lectures, or content addressed in sciences/biology classes, and health professionals, with the dentist being the most cited (Graph 1).
A very low frequency (27.9%; n = 320) stated that they had heard about the self-examination of the oral cavity for the detection of signals that may be related to oral cancer. And among these subjects, only 17.5% (n = 56) had performed selfexamination.
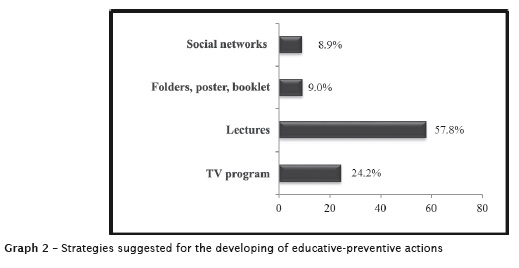
When they were asked if they would like to participate in educational and preventive activities on oral cancer and other thematic related to health, the majority (72.6%; n = 834) showed interest. When inquiring about the strategies they considered important for the development of educational and preventive activities, most reported lectures (Graph 2).
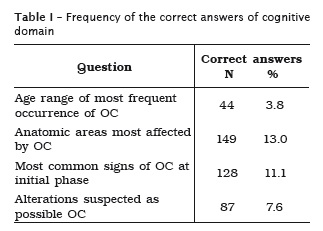
Regarding the level of knowledge, the percentage of correct answers was very low, ranging from 3.8% to 13%, on the questions related to signs/ symptoms, location and age of occurrence of oral cancer (Table I).
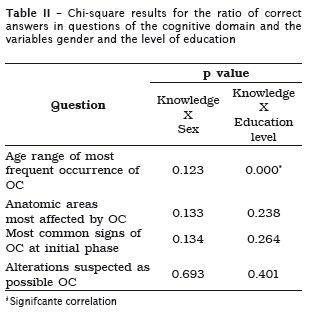
To this set of questions no significant association was found, by Chi-square test, between the level of knowledge (defined by the frequency of correct answers) and sex of respondents (Table II). When we analyzed the association between level of knowledge and level of education (the last year of elementary school and junior high school), a significant association was found (p < 0.01), by Chi-square test, only to the question "What is the most frequent age of occurrence of oral cancer?" (Table II), showing a better understanding of high school subjects, in this question.
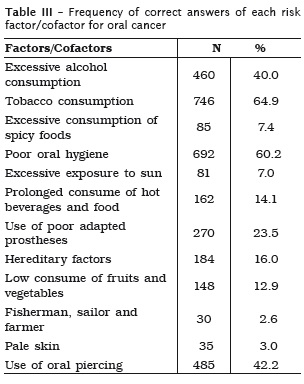
In the question of risk factors and cofactors related to oral cancer, among the 12 listed alternatives, only tobacco and poor oral hygiene items, the correct answer rate was just over 50% (Table III).
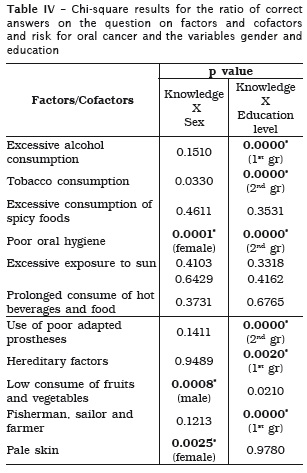
The association between level of knowledge and sex and educational level was significant (p < 0.01), by Chi-square test in some of the items listed (Table IV).
The classification of the knowledge level of the group on oral cancer, according to the criteria established in this present study, was between regular and unsatisfactory, as it can be seen in graph 03.
Discussion
The fight against cancer has been growing in recent years. However, unfortunately, all over the world, 50% of patients with oral cancer are at an advanced stage. Among the factors that may be associated to the problem and justify the high percentage of late diagnosis is: poor training in this area and population's lack of knowledge about the disease1,3,24,25.
The understanding of the risk factors and cofactors, the natural history and epidemiology of oral mucosa lesions is essential to promote primary prevention, early diagnosis, and proper planning of health services. The guarantee of health education programs aimed at general population screening, appropriate treatment, and quality of life associated with the improvement of knowledge of health professionals on oral cancer are needed to reduce the morbidity and mortality resulting from this neoplasia1,3,4,7,12,16,19,20,21,26,27.
The recognition, by the population, of the risk factors and cofactors, the most common signs and symptoms at the early stage of the disease, and the importance of early diagnosis, is essential to lower rates of cases of oral1,4,5,14,19,26. However, in the population studied, the frequency of subjects that inform had received information, known, or have carried out self-examination of the oral cavity for the detection of signals that may be related to oral cancer was very low.
The assessment of knowledge of these subjects was seen as a motivating and mobilizing element of the target population as they noted the need to increase their knowledge on the subject of oral cancer and analyze the care they routinely engaged in oral health. Thus, we consider as a guiding principle of this research the Primary Health Care based on educational activities, governed by the principles of health promotion. Therefore, the discussion developed based on this perspective.
One aspect that should be highlighted is the age profile of the target population. Because they are young, it is considered that they are much more vulnerable to the action of environmental factors, especially those related to habits and lifestyles. It is therefore unquestionably the importance of giving attention to this group and by analyzing which information they have in order to enhance educational and preventive activities.
On the literature reviewed, there is a consensus that the primary prevention of disease, through an educational process, can contribute to the awareness of the people. Knowledge influences the behavior at all social levels of organization. Lack of awareness of individuals about signs, symptoms and risk factors associated with oral cancer is a powerful barrier to early detection1-5,7,11,13,14,16,19-23,26,27.
The transmission of basic information can strengthen the population's ability to deal with health problems. The acquired knowledge allows the subjects to be able to make choices that promote health or predispose to disease. In this context, knowledge about the development of malignancies is essential to prevention. Notwithstanding, researches have shown that there is a significant lack of knowledge of the population in general about the risk factors/cofactors for oral cancer14,16,19,21,26, 27.
The results of this present study indicated that the knowledge of the respondents on the subject of oral cancer is unsatisfactory, confirming the findings reported in studies conducted in different contexts14,16,19,21,26,27. It is noteworthy, in this study, the low percentage of correct answers on the factors associated with oral cancer, which are already established in the literature, such as sunlight, tobacco, and alcohol.
With regard to the consumption of tobacco and alcohol as risk factors associated with oral cancer, although they were the most cited by the subjects of this research, the rate of correct answers was low because fluctuated between regular and unsatisfactory levels. This result deserves attention because according to the Brazilian Survey on the Scholar Health10, the higher frequency of experimentation of this two risk factors among adolescents was observed in the south region.
Concerning to exposure to sunlight and related conditions, such as certain professions and paleskin people who are part of the risk group for developing oral cancer, it was observed that few subjects that related that to oral cancer. This finding is very worrying, because the studied population lives in a coastal region.
The literature is consistent with regard to the etiology of oral cancer, noting that the disease results from a sum of carcinogenic factors, and key are extrinsic, such as smoking, alcohol, and chronic exposition to sunlight3,4,6,7,12,13,15,18,19,12-27. However, other factors can contribute to the development of oral cancer, although the literature is not yet clear. Consequently, the unsatisfactory level of correct answers for factor/cofactors as: excessive consumption of spicy foods, prolonged use of drinks and hot food, use of poor-fitting dentures, low consumption of fruits and vegetables did not prove out the expectations of the researchers.
Currently, there are records that poor oral hygiene, poorly fitting dentures, broken teeth or dental remains, over the years, are causes of hyperplastic lesions, and therefore, the constant and long action of these oral conditions can be a cofactor for development of oral cancer, by favoring the action of other carcinogens, particularly tobacco and alcohol2,6,15,18,19,22.
Other behaviors also have been linked to oral cancer. Current knowledge has emphasized the important role of diet in cancer etiology. Studies have shown that nutritional deficiencies and inadequate diets act as sources of free radicals, which would be responsible for alterations in DNA and can foster the development of oropharyngeal cancer. Fruits and vegetables probably can reduce the risk of cancer of the oral cavity6,2,12,13,15,22. And the consumption of hot beverages or foods due to thermal injury to mucosal cells can increase oral cancer risk, even though few conclusive studies have been carried out 2,3,12,22.
The low level of knowledge about oral cancer evidenced by volunteers in this study probably is related to the fact that most had never received information on the subject. To reverse this situation it is suggested to offer campaigns on the subject, in accessible language, because of the very high percentage of respondents expressed interest in receiving instructions on this and other themes related to health and pointed out the lecture as the preferred strategy for the information transfer.
Although there is no conclusive studies on the impact of primary prevention strategies23, many researchers1-8,12,13,16,19-22,24-27 admit that it is necessary to increase public awareness about cancer and precancerous lesions, including knowledge about the risk factors.
Information campaigns in the media, according to Van Der Waal et al.24, have little effect; however, the distribution of leaflets can be very useful. Among the participants of this present study, this assertion is corroborated, since many of those who had received information reported educational materials as a major source available in the basic health units.
The problem regarding to this strategy type is that the specific educative materials on the oral cancer are still few and those available generally are in a language not accessible to the understanding of the lay population19,20,24,27. Ent Thus, there is a failure to produce this material type to be shown among the population, so it is necessary that the professionals responsible for preparing the material to consider the population level with which they will work.
As evidenced by Herr et al.7, it is important that professionals of health services act in different social spaces, spreading accessible technical and scientific knowledge, and demystifying the disease, because the more informed the population are, the greater is the possibility to enable the identification of risk factors and to seek the prevention and diagnosis.
It should be noted that, although the nonprobability sampling design used in this study might be considered a limitation, our understanding is that the sample size and the fact that these subjects coming from different geographical areas of the city are factors that minimize the possibility of a bias in the selection of subjects. Therefore, we believe that the results can be extrapolated to the entire school population of the public school system in the city where the research took place. We also understand that the reality identified in this youth group should be occurring in other contexts of Santa Catarina, as well as in other regions of the country.
Given this reality and the positive attitude of respondents as to obtain more knowledge on the subject, the research team has developed lectures with distribution brochures to and the students comprising the target population. Therefore, the research motivated the scholars regarding the acquisition of knowledge that promote attitudes for prevention of oral cancer.
Finally, we point out that these data can be used by city managers responsible for planning educational and preventive actions, strengthening the work already begun with the subjects researched and extending it to the entire population.
Conclusion
Based on the obtained results, it can be concluded that the students of the Public school system in the city of Itajaí do not have adequate knowledge on oral cancer.
Acknowledgements
The authors thank the Program of Research Fellowship, Article no. 171/FUMDES/ Government of the State of Santa Catarina.
References
1. Almeida FCS, Silva DP, Amoroso MA, Brito e Dias R, Crivello Junior O, Araújo ME. Popularização do autoexame da boca: um exemplo de educação não formal – parte II. Ciênc Saúde Coletiva. 2011;16(supl.1):1589-98.
2. Brasil. Ministério da Saúde. Secretaria de Assistência à Saúde. Instituto Nacional de Câncer – INCA. Falando sobre câncer da boca. Rio de Janeiro: INCA; 2002.
3. Dib LL, Souza RS, Tortamano N. Avaliação do conhecimento sobre câncer bucal entre os alunos de Odontologia, em diferentes unidades da Universidade Paulista. Rev Inst Ciênc Saúde. 2005 Oct-Dec;23(4):287-95.
4. Elango KJ, Anandkrishnan N, Suresh A, Iver SK, Kuriakose MA. Mouth self-examination to improve oral cancer awareness and early detection in a highrisk population. Oral Onc. 2011;47(7):620-4.
5. França DCC, Pinto MMO, Monteiro AD, Silva AAS, Zina O, Lima GS et al. Programa de diagnóstico e prevenção de câncer de boca: uma estratégia simples e eficaz. ROBRAC. 2010;19(49):159-61.
6. Garrote LF, Herrero R, Reyes RM, Vaccarella S, Anta JL, Ferbeye L et al. Risk factors for cancer of the oral cavity and oro-pharynx in Cuba. Br J Cancer. 2001;85:46-54.
7. Herr GE, Kolankiewicz ACB, Berlezi EM, Gomes JS, Magnago TSBS, Rosanelli CP et al. Avaliação de conhecimentos acerca da doença oncológica e práticas de cuidado com a saúde. Rev Bras Cancerol. 2013;59(1):33-41.
8. Hertrampf K, Wenz HJ, Koller M, Grund S, Wiltfang J. Early detection of oral cancer: dentists’ opinions and practices before and after educational interventions in Northern-Germany. J Craniomaxillofac Surg. 2013;41(8):e201-7.
9. Instituto Brasileiro de Geografia e Estatística. Cidades@ [cited 2013 Nov 26]. Available from: URL:http:// www.cidades.ibge.gov.br/xtras/home. php.
10. Instituto Brasileiro de Geografia e Estatística. Pesquisa Nacional de Saúde do Escolar 2012. Rio de Janeiro: IBGE; 2013 [cited 2013 Nov 26]. Available from: URL:http://www.ibge.gov.br/home/estatistica/ populacao/pense/2012/pense_2012.pdf.
11. Jung M. Cancer control and the communication innovation in South Korea: implications for cancer disparities. Asian Pacific J Cancer Prev. 2013;14(6):3411-7.
12. Key TJ, Schatzkin A, Willett WC, Allen NE, Spencer EA, Travis RC. Diet, nutrition and the prevention of cancer. Public Health Nutr. 2004;7(1A):187-200.
13. Leite ACE, Guerra ENS, Melo NS. Fatores de risco relacionados com o desenvolvimento do câncer bucal: revisão. Rev Clín Pesq Odontol. 2005;1(3):31-6.
14. Melo AUC, Ramalho LMP, Ribeiro CF, Rosa MRD. Informação e comportamento preventivo de pacientes do Programa de Saúde da Família de Aracaju a respeito de câncer de boca. Pesqui Bras Odontopediatria Clín Integr. 2012;12(3):377-82.
15. Meurman JH. Infectious and dietary risk factors of oral cancer. Oral Oncol. 2010;46:411-3.
16. Parizi JLS, Castro SD, Ponga CMQ, Parizi AGS. Conhecimento de acadêmicos de odontologia, cirurgiões-dentistas e população em geral sobre câncer de boca. Rev Assoc Paul Cir Dent. 2011;65(1):66-70.
17. Rahman B, Hawas N, Rahman MN, Rabah AF, Kawa S. Assessing dental students’ knowledge of oral cancer in the United Arab Emirates. Int Dent J. 2013;63(2):80-4.
18. Rosenquist K. Risk factors in oral and oropharyngeal squamous cell carcinoma: a population-based case-control study in southern Sweden. Swed Dent J Suppl. 2005;179:1-66.
19. Souza LRB, Ferraz KD, Pereira NS, Martins MS. Conhecimento acerca do câncer de boca e atitudes frente à sua etiologia e prevenção em um grupo de horticultores de Teresina (PI). Rev Bras Cancerol. 2011;52(1):31-9.
20. Srikanth Reddy B, Doshi D, Padma Reddy M, Kulkarni S, Gaffar AAM, Reddy V. Oral cancer awareness and knowledge among dental patients in South India. J Craniomaxillofac Surg. 2012;40(6):521-4.
21. Tadbir AA, Ebrahimi H, Pourshahidi S, Zeraatkar M. Evaluation of levels of knowledge about etiology and symptoms of oral cancer in southern Iran. Asian Pacific J Cancer Prev. 2013;14(4):2217-20.
22. Toporcov TN, Biazevic MGH, Rotundo LDB, Andrade FP, Carvalho MB, Brasileiro RS et al. Alimentos de origem animal e câncer de boca e de orofaringe. Rev Panam Salud Publica. 2012;32(3):185-91.
23. Torres-Pereira C, Angelim-Dias A, Melo NS, Lemos Jr CA, Oliveira EMF. Abordagem do câncer da boca: uma estratégia para os níveis primário e secundário de atenção em saúde. Cad Saúde Pública. 2012;28(Supl.):s30-9.
24. Van der Waal I, De Bree R, Brakenhoff R, Coebergh J. W. Early diagnosis in primary oral cancer: is it possible? Med Oral Patol Oral Cir Bucal. 2011;16(3):e300-5.
25. Van der Waal I. Are we able to reduce the mortality and morbidity of oral cancer: some considerations. Med Oral Patol Oral Cir Bucal. 2013;18(1):e33-7.
26. Vidal KL, Tenório APS, Brito BHG, Oliveira TBT, Pessoa ID. Conhecimento de escolares do sertão pernambucano sobre o câncer de boca. Pesqui Bras Odontopediatria Clín Integr. 2009;9(3):283-8.
27. Zanetti F, Azevedo MLC, Perez DEC, Silva SRC. Conhecimento e fatores de risco do câncer de boca em um programa de prevenção para motoristas de caminhão. Odontol Clín-Cient. 2011;10(3):233-41.
 Corresponding author:
Corresponding author:
Elisabete Rabaldo Bottan
Curso de Odontologia – Grupo de Pesquisa Atenção à Saúde Individual e Coletiva em Odontologia
Universidade do Vale do Itajaí Rua Uruguai, n. 458 – Centro
CEP 88302-202 – Itajaí – SC – Brasil
E-mail: erabaldo@univali.br / erabaldo@gmail.com
Received for publication: February 28, 2014
Accepted for publication: September 2, 2014
