










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRSBO (Online)
versão On-line ISSN 1984-5685
RSBO (Online) vol.12 no.1 Joinville Jan./Mar. 2015
Original Research Article
Evaluating of oral and salivary conditions of two specific groups of workers
Nicolae Carvalho de PaulaI; Carolina Dea BruzamolinI; Paulo H. TomazinhoI; Luciane Variani PizzattoI; Wellington M. ZaitterI; Eduardo PizzattoI
I School of Dentistry, Positivo University – Curitiba – PR – Brazil
ABSTRACT
Introduction and Objective: Tooth decay is one of the most common chronic oral diseases found in industrial countries and is a multifactorial disease which has sugar as a key dietary factor. The amount of saliva concentration and presence of cariogenic bacteria will favor the development of caries. Because of this, the aim of this study was to collect and analyze data on oral alterations referred to tooth decay, oral pH changes, and changes of the oral microbiota in two distinct groups of workers. Material and methods: 30 individuals belonging to two different groups of workers: group A (GA) – workers who maintain daily contact with the confectionery; group B (GB) – workers who do not have such contact. Saliva collection was done by analysis of the salivary pH in both groups, as well as cultivation of Lactobacillus spp and S. mutans. We also evaluate the dental status of individuals belonging to the two groups through the DMFT index. Results: After the examinations of 30 workers (17 from the GA [9 men and 8 women] and 13 in the GB [7 men and 6 women]), the mean DMFT of the individuals in the group A and group B, was 7.41 (SD 5.14) 7.08 (SD 5.56), respectively, without statistically significant differences (p < 0.05). The count of S. mutans and Lactobacillus spp, was not statistically significant. Conclusion: There was no statistically significant relationship between presence of dental caries and the fact that workers are in contact with sugar because they work on candy food industry, but new studies are needed for more precise research.
Keywords: oral health; occupational dentistry; DMF index; saliva.
Introduction
Tooth decay is one of the chronic oral diseases more common found in industrial countries. Despite the reduction in the severity and prevalence of the disease, caries still has gradually increased with age and remains a problem of public health 15. Dental caries is a multifactorial disease and occurs due to the diet, negligent oral hygiene, biofilm maturation time, and the presence of acids and bacteria in the oral cavity 6,10.
The dietary factor known as major cause of tooth decay is sugar. This is associated with the presence of acids in the mouth by the action of bacteria, causing a process of dissolution and mineral loss of dental enamel 10,11. In the study of Sigh et al. 16 there was a correlation between exposure to sugar with caries incidence in workers with and without dental health insurance in India. The oral health was assessed and a survey on social-demographic factors, including: exposure to sugar, smoking, and oral hygiene habits. It was found that workers who had frequency of exposure to sugar of three or more times a week were shown to have a higher caries incidence than workers who had no exposure.
Saliva has a fundamental role in the oral cavity maintenance, because acts as a buffer solution to neutralize the acids from attack of bacteria produced during sucrose fermentation, so that the oral environment becomes neutral. Thus, the adhesion of bacteria on tooth surface and a possible loss of minerals, calcium and phosphate are avoided 6,10,17.
Streptococcus mutans, the main bacterium that causes dental caries, is an extracellular and acidogenic bacterium inducing dental caries in humans with a high-sucrose diet. The presence of S. mutans in the oral cavity, associated to poor hygiene and high consumption of carbohydrates, favors acidogenesis, triggering the carious lesions initially in dental enamel 10,12,18. For a better determination of the patient's risk to develop caries, some tests have been performed: salivary test (to check flow and salivary pH) and bacterial count (which is done by counting bacterial colonies forming units) 6,17.
This research is justified because there is no evidence of dental caries and salivary change caused by the work environment in the confectionery industry workers. The aim of this study was to collect and analyze data on oral alterations referred to caries, oral pH changes, and changes in the oral microbiota in two groups: candy industry and real estate workers.
Material and methods
Previously, this study was evaluated and submitted to the Ethics Committee in Research of Positivo University, according to Resolution n. #196/96. A total of 30 workers of two distinct groups were evaluated: Group A (GA) – workers who maintain daily contact with sweet production; and Group B (GB) – workers who do not have such contact. The age group of the subjects in both groups was matched in 18-45 years with working time over six months on the activity and did not use orthodontic appliances.
Caries assessment
The clinical intraoral examination performed in the sample group followed the model recommended by the World Health Organization (WHO). The following variables were evaluated: age, sex, length of stay in employment and dental caries (this through the DMFT index) 11.
That exam was performed with the aid of n. 5 flat mirror, WHO periodontal probe, and wooden spatula. These objects made up kits that were opened only at the time of the examination, passing through a washing process and autoclaving at the end of the day. The data were recorded in individual medical records. These tests were performed in-house, by a single calibrated examiner under natural light, with the person sitting and the examiner standing. It is noteworthy that the diagnosis, during the intraoral examination of pathological conditions, especially triggering of nociceptive processes, received referral to clinical treatment.
It is worth noting that prior contact was conducted explaining the objectives of this study and protocol of the examinations sent to person in charge of each company in order to obtain necessary authorization to perform this research. Moreover, all workers signed a free and clarified consent form to undergo intraoral examination.
The data collected during the diagnosis phase were entered into the statistical program Epibuco produced in Fox Base language, which were tabulated and received statistical treatment. For comparison between groups we used analysis of variance – ANOVA.
Salivary collection
Two to three hours after last oral hygiene, a sterile cotton roll has been chewed for 1 minute and the saliva produced was swallowed. The saliva produced thereafter was collected by sputum for 3 minutes in sterile plastic vial. The vials containing the saliva were stored in Styrofoam box with crushed ice and transported to the Microbiologic Laboratory of Positivo University.
Determination of salivary pH
With the saliva samples in the Microbiology Laboratory of Positivo University, a 1 ml aliquot was removed from each sample and packaged under 1.8 ml sterile disposable plastic Eppendorff tubes for further saliva analysis. After this procedure, the saliva remaining in each collection flask had the pH determined by pH meter, previously calibrated with pH buffers from 4 to 7.
Lactobacillus spp and S. mutans cultivation
For S. mutans cultivation, 0.5 ml aliquots of saliva from each individual were homogenized and serial diluted in 4.5 ml of saline solution, 0.85% by 1:10000 dilution. After dilution, 0.1 ml aliquots of each dilution were plated on Agar Mitis Salivarius culture media supplemented with 20% sucrose. The plates were incubated in a bacteriological incubator (FANEM, Sao Paulo, Brazil) at 37°C for 48 hours, after which the colonies grown were counted under a stereoscopic microscope to determine the unit forming colony per ml of saliva (CFU/ml) (figure 1).
For cultivation three kits with Rogosa agar (DENTALLABOR, Pinhais, Brazil). For that, the remaining of saliva sample was pipetted with disposable Pasteur pipette and saliva aliquots were spread on the lateral side of the pipette itself on the agar. The tubes containing the culture were also incubated at 37ºC for 48 hours (figure 2).
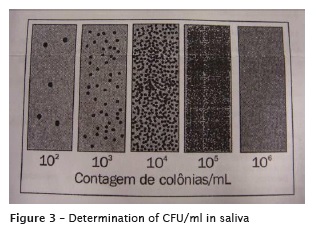
After the growth period on the medium surface was compared with template supplied by the manufacturer to determine the amount of CFU/ml in saliva (figure 3).
Statistics
The means of the groups were statistically analyzed by Epibuco software, at significance level of 5%. The Student t test was used to verify the statistical differences between the groups.
Results
Thirty workers were examined: 17 of GA (9 men and 8 women) and 13 of GB (7 men and 6 women). The mean DMFT of the individuals of GA was 7.41 (SD 5.14) and GB was 7.08 (SD 5.56). However, this difference was not statistically significant (p<0.05) (tables 1 and 2).


Discussion
At the working environment, there is exposure to various diverse factors that may cause damage to human health. Because of this, depending on the nature of the damage suffered by the worker, severe damage to oral health might occur 19.
The Dentistry at Work covers the worker's health as a priority and seeks to find possible factors that may cause disease. However, there are few current studies in the literature that address the Dentistry at Work and worker risk. Therefore, current studies should be conducted and Dentistry must have a deeper look in relation to oral health of worker.
The methods and materials used in the study were very efficient, since, in the obtaining results, there was only time problem between the saliva collection and analysis of the obtained material. The inf luence of saliva buffer capacity was an important factor to indicate the restoration of oral pH to both GA (mean pH 7.99) and G B (mean pH 7.67), which demonstrates that the result of oral pH values changed 18.
There was no statistical difference in the results obtained in S. mutans and Lactobacillus spp count. It is said in some studies that the count may have certain limitations, because other predisposing factors must be taken into consideration for the development of caries, such as biofilm maturation, time, poor hygiene and cariogenic diet 6.
A study conducted in 1978 veri f ied the prevalence of dental caries in workers of candy factories in Israel and compared with workers of textile industries. Values found in workers of candy industries were significantly higher than those of the other group, suggesting the need for special attention to workers exposed to air sugar 1.
A survey carried out the assessment in the confectionery industry workers, separated into groups: Chocolate, sweet biscuits, bakery, and sweets. Through clinical oral examination, it was found that workers of chocolates and cookies had higher caries, with a higher incidence in those who are in employment for longer and in confectioners who are exposed to sugar 4-6 hours a day. Some workers, in addition to caries, already had periodontal disease and needed treatment and more efficient control of oral diseases 14.
The statistical equality in DMFT index of the two groups is also due to the average of decayed teeth to be 2.41 in the GA and 0.92 in B and the average of restored teeth in GA to be 3.47 and in GB 4.62. These means directly altered DMFT result of the two groups, which demonstrated greater activity of caries in GA, which is exposed to sugar, and greater amount of restorations in Group B.
It is assumed that workers of chocolates industries, chewing gum, and sugar are daily exposed to fine particles of raw materials suspended in the air, such as f lour, refined sugar and sweeteners. A study was carried out to assess the incidence of caries in a group of exposed and unexposed workers, but it was not observed relation in DMFT increase resulting from exposure to sugars 20.
By evaluating the oral health status of workers in a confectionery industry in Denmark, Petersen 13 concluded that these form a risk group for dental caries, being necessary to establish a preventive oral health program as part of the occupational health program of the company. A study on Chinese airline pilots showed that pilots consumed sugar more frequently and had higher caries index than those that did not consumed. But there was no significance difference between exposure to sugar and caries, because pilots often underwent dental visits 12.
Masalin et al. 7 evaluated the oral health conditions of 298 workers in candy factories of Finland, concurrently assessed the concentrations of sugar and flour in the workplace, which were within the accepted limits. The researchers concluded that the consumption of sugary products, the frequency of use, and the behavior of workers in relation to oral health are the main responsible factors for the high rates of dental problems in these workers.
Masalin et al. 8 analyzes the state of dental caries, food behavior, and oral health. In salivary microbiological discoveries of 338 confectionery workers, caries experience was found in high quantities. Food habits were the most important factors affecting the occurrence of caries and its susceptibility. The authors concluded that the confectionery industry did not seem to be an extremely dangerous environment for oral health in general.
Conclusion
Based on the results, it can be concluded that
• In the specific groups of workers statistically significant difference was not proven between the studied variables;
• Due to the lack of current literature, further studies should be conducted to analyze the correlation of oral diseases and exposure to occupational hazards by workers;
• It is suggested further studies following the proposed methodology, using a more significant sample group in order to verify that the results obtained here are reproducible.
References
1. Anaise JZ. Prevalence of dental caries among workers in the sweetes industry in Israel. Community Dent Oral Epidemiol. 1978;6(6):286-9. [ Links ]
2. Carvalho VA, Espindula MG, Valentino TA, Turssi CP. Approaches used in the assessment of caries risk. RFO. 2011 Jan-Apr;16(1):105-9.
3. Chen X, Liu Y, Yu Q, Zheng L, Hong X, Yan F et al. Dental caries status and oral health behavior among civilian pilots. Aviat Space Environ Med. 2014 Oct;85(10):999-1004.
4. Hics J, Garcia-Godoy F, Flaitz C. Biological factors in dental caries: role of saliva and dental plaque in a dynamic process of demineralization and remineralization. J Clin Pediatr Dent. 2003;28:47-52.
5. Kalesinskas P, Kacergius T, Ambrozaitis A, Peciuliene˙ V, Ericson D. Reducing dental plaque formation and caries development. A review of current methods and implications for novel pharmaceuticals. Stomatologija, Baltic Dental and Maxillofacial Journal. 2014;16(2):44-52.
6. Kidd EAM, Fejerskov O. What constitutes dental caries? Histopathology of carious enamel and dentin related to the action of cariogenic biofilms. J Dent Res. 2004;35-8.
7. Masalin K, Murtomaa H, Meurman JH. Oral health of workers in the modern finnish confectionery industry. Community Dent Oral Epidemiol. 1990;3(18):126-30.
8. Masalin KE, Murtomaa HT, Sipila KP. Dental caries risk in relation to dietary habits and dental services in two industrial populations. Journal Public Health Dent. 1994;3(54):160-6.
9. Midorikawa ET. Definição do campo de atuação e funções do cirurgião-dentista na equipe da saúde do trabalhador. Revista CIPA. 2001 May;(258):52-69.
10. Moynihan P. The interrelationship between diet and oral health. Proc Nutr Soc. 2005;64:571-80.
11. Organização Mundial de Saúde. Levantamento epidemiológico básico em saúde bucal: manual de instruções. 4. ed. Genebra: OMS; 1999.
12. Pereira AG, Neves AM, Trindade AC. Imunologia da cárie dentária. Acta Med Port. 2010;23:663-8.
13. Petersen PE. Evaluation of a dental preventive program for Danish chocolate workers. Community Dent Oral Epidemiol. 1989(17):53-9.
14. Rekha R, Hiremath SS. Oral health status and treatment requirments of confectionery. 2002;13(3-4):161-5.
15. Sheiham A, James WP. A reapraisal of the quantitative relationship between sugar intake and dental caries: the need for new criteria for developing goals for sugar intake. BMC Public Health. 2014 Sep 16;14(1):1-8.
16. Singh A, Purohit BM, Masih N, Kahndelwal PK. Risk factors for oral diseases among workers with and without dental insurance in a national social security scheme in India. Int Dent J. 2014;64(2):89-95.
17. Struz˙ y cka I . The oral microbiome in dental caries polish. Journal of Microbiology. 2014;63(2):127-35.
18. Takahashi N, Nyvad B. The role of bacteria in the caries process: ecological perspectives. J Dent Res. 2011 Mar;90(3):294-303.
19. Tannous RA, Silva UA. Revisão de literatura – Odontologia do trabalho: aplicabilidade e importância na saúde bucal do trabalhador. UFES Rev Odontol. 2007 Sep-Dec;9(3):43-8.
20. Tomita NE, Cordeiro R, Mendonça J, Senger V, Lopes ES. Saúde bucal dos trabalhadores de uma indústria alimentícia de centro-oeste paulista. Rev FOB. 1999;7(1/2):67-71.
 Corresponding author:
Corresponding author:
Eduardo Pizzatto
Rua Professor Pedro Viriato Parigot de Souza, n. 5.300 – Campo Comprido
CEP 81280-330 – Curitiba – PR – Brasil
E-mail: epizzatto1@gmail.com
Received for publication:
Accepted for publication:
