










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRSBO (Online)
versão On-line ISSN 1984-5685
RSBO (Online) vol.12 no.1 Joinville Jan./Mar. 2015
Case Report Article
Compound odontoma associated with dentigerous cyst in the anterior mandible – case report
Radamés Bezerra MeloI; Yuri Edward de Souza DamascenoII; Celio Armando Couto da Cunha JuniorIII; Igor Vasconcelos PontesIV
I Department of Surgery, Federal University of Ceará – Fortaleza – CE – Brazil
II Department of Odontology, Federal University of Pará –Belém – PA – Brazil
III Department of Oral and Maxillofacial Surgery, University Hospital João de Barros Barreto – Belém – PA – Brazil
IV Department of Oral and Maxillofacial Surgery, Hospital Batista Memorial – Fortaleza – CE – Brazil
ABSTRACT
Introduction:The dentigerous cyst, also called a follicular cyst is an odontogenic cyst that develops in association with crown of an impacted tooth, predominantly in mandibular third molars of young patients. The Odontoma is a ectomesenquimal tumor of unknown origin that are more considered developmental malformations (harmatomas) than benign neoplasms. Occasionally, the dentigerous cyst is associated with odontoma. Objective:The article aims to report a case of surgical treatment of dentigerous cyst associated with compound odontoma and unerupted tooth in anterior region of the mandible. Case report: A male patient, 17 years of age, without systemic changes, was sent to the Center for Dental Specialties of Horizonte, Ceará, Brazil, specialty of Oral and Maxillofacial Surgery, for diagnosis and treatment of oral lesions visualized after periapical radiographic examination to determine failed eruption of element 42. Observing the periapical radiograph it was possible to visualize radiopaque lesion suggestive of a compound odontoma and a cystic capsule in association with the element 42. A panoramic radiograph was requested and it was planned a surgical removal of odontoma with curettage of bone cavity and removing the cystic capsule and element 42. There were no significant postoperative complications, the suture removal was performed 7 days after surgery where it was possible to observe a good healing, no swelling and no paresthesia. Conclusion: The treatment of choice is surgical excision of the lesions with the tooth associated to the cyst, it should be performed with proper planning, avoiding injury to vital structures and should not be delayed in order to avoid possible occlusion sequelae.
Keywords: intraosseous; lesions; diagnosis; surgery, oral.
Introduction
The dentigerous cyst, also called a follicular cyst is an odontogenic cyst that develops in association with crown of an impacted tooth, predominantly in mandibular third molars of young patients. Lesions are often asymptomatic unless associated with an infectious process and is generally diagnosed in routine radiographs6.
The radiographic features of dentigerous cyst shows a radiolucent area with sclerotic border well defined and attached to the neck of the tooth unerupted. May be accompanied by tenderness, swelling, tooth mobility or tooth displacement when it reaches the diameter of 2 cm1.
Occasionally, the dentigerous cyst is associated with impacted teeth or odontoma. Its association with odontoma is seen in 27.6% of cases7.
The Odontoma is aectomesenquimal tumor of unknown origin, may be related to the presence of impacted teeth, trauma, local infection and dentigerous cysts14. Among odontogenic tumors, odontoma is the most prevalent in the jaws9, representing 70% of odontogenic tumors found8,2,16, are more considered developmental ma l format ions (ha rmatomas) than benig n neoplasms.
The article aims to report a case of surgical treatment of dentigerous cyst associated with compound odontoma and unerupted tooth in the anterior region of the mandible.
Case report
A male patient, 17 years of age, without systemic changes, was sent to the Center for Dental Specialties of Horizonte, Ceará, Brazil, specialty of Oral and Maxillofacial Surgery, for diagnosis and treatment of oral lesions visualized after periapical radiographic examination to determine failed eruption of element 42. Observing the periapical radiograph it was possible to visualize radiopaque lesion suggestive of a compound odontoma, being possible to view multiple denticles.
Panoramic radiograph and clarck technique was requested for better visualization of the lesions and the location of the element 42 (figure 1).
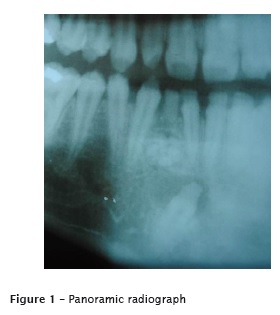
It was planned a surgical act to remove the odontoma with curettage of bone cavity and removing the cystic capsule and element 42, because the element was found badly positioned with proximity to the roots of the elements 41 and 42, risking of root resorption in the attempted traction.
To complement the surgical plan, the Clark technique was realized to found that the Odontoma and element 42 would be best addressed by the vestibular access, due to its position in front of the roots of the mandibular anterior teeth.
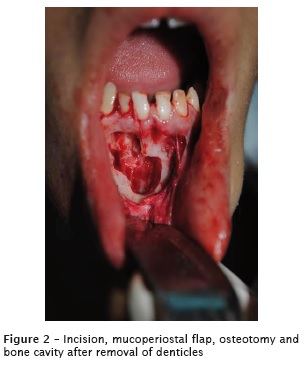
The surgical protocol consisted of extra oral antisepsis performed with povidone iodine topical (Riodeine®) and intraoral performed with chlorhexidinegluconate 0.12%; regional anesthesia by blocking the bilateral mental nerve and complementation with infiltrative techniques. The Novak-Peter incision was made in the region of element 43 to 41. After detashment the mucoperiosteal flap, it was performed an osteotomy with surgical round burs in high rotation under irrigation with saline 0.9% for access to denticles and the element 42, which were removed with straight and curved extractors (figures 2 and 3). The flap was repositioned, and the suture was performed by simple sutures isolated.

The patient was properly instructed to the postoperative care and medicated with corticosteroids, antibiotics, analgesic and anti-inflammatory. There were no significant postoperative complications, the suture removal was performed 7 days after surgery where it was possible to observe a good healing, no swelling and no paresthesia (figure 3).

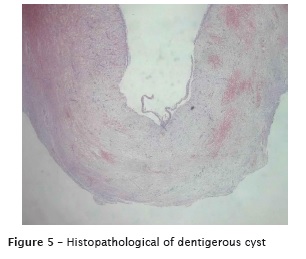
The cystic material was sent for histopathological analysis, which indicated a squamous epithelial tissue with 2-4 layers surrounded by a capsule of fibrous connective tissue, confirming the hipothesis of dentigerous cyst (figure 4).
Discussion
The World Health Organizat ion in 1992 ranked the odontomas into two types, according to morphological differentiation: compound and complex5. The compound odontoma was defined as an injury that stems from an exaggerated proliferation of the dental lamina, showing all dental tissues in an orderly manner and are often presented in the form of denticles. Radiographically can characterize the compounds odontoma as a set of structures similar to the teeth, may have a variable sizes and shapes, surrounded by a radiolucent area. In the complex odontoma, dental tissues are found like an amorphous calcified mass and radiographically visualized by a uniform radiopacity with irregular edges surrounded by radiolucent space18.
The odontomas are detected most commonly in the first two decades of life, with no gender predilection 4. There is a higher frequency of compound odontoma comparing to the complex and the most frequent location of compound odontoma is the anterior region of the maxilla, and complex odontoma the posterior regions of the jaws2,12,15.
In most cases the lesions are asymptomatic, although they may cause thickening of the cortical, being discovered on routine radiographic examination or to determine the reason for an eruption failure of a particular tooth, like in this case3.
Odontomas may be associated with delayed eruption of permanent teeth and the development of cystic lesions such as dentigerous cyst. These cases are not rare (27.6%) and the diagnosis is based on radiological aspects and histopathological analysis of the lesions, in some cases radiological aspects may resemble fibro-osseous lesions17.
This case shows a compound odontoma evidenced in imaging exams by multiple denticles encircled and a radiolucent area in anterior region of mandible associated a dentigerous cyst in the anterior region of the mandible. The surgical exposure showed the cystic lesion attached to the neck of the tooth unerupted.
The dentigerous cyst predominantly affects mandibular third molars of young patients, followed by maxillary canine, mandibular premolar and maxillary third molar. It is usually asymptomatic and may be associated with mobility or displacement of teeth, radiographically characterized by a radiolucent lesion with a well-defined sclerotic margin associated with a crown of a tooth unerupted1,10. Histopathological consists of a fibrous conjunctive tissue capsule and an epithelial lining of two to four layers of flattened cells may or may not present a keratinized surface13.
Complications associated with dentigerous cysts are pathological bone fracture, loss of permanent teeth, bone deformit ies and development of ameloblastoma or malignancies such as squamous cell carcinoma and intraosseousmucoepidermoid carcinoma7,10,13.
The treatment of odontoma is surgical excision, such treatment has great success with very rare cases of recurrence, occurring bone repair15. The indicated treatment for dentigerous cysts is surgical excision with removal of the involved tooth, in some cases may be necessary marsupialization of the lesion for the reduction of bone defect before surgical intervention10.
This case was treated by surgical excision of the lesions and the associated tooth. The choice of surgical traction of the unerupted tooth was avoided because of its difficult location and possibility of resorption of adjacent elements. The size of the lesion did not require marsupialization before removal and the patient remained with a satisfactory amount of surrounding bone.
The diagnosis of the lesions is done mainly by initial imaging exams and subsequently confirmed by histopathological analysis. The failure to diagnose or treatment can lead to disorders ranging from aesthetic and phonetic until drastic occlusal changes19.
Conclusion
The compound odontoma is benign malformation that the diagnosis is clinical and radiographic, usually asymptomatic, with slow evolution and may be associated with other disorders such as dentigerous as outlined in this case. The treatment of choice is surgical excision of the lesions with the tooth associated to the cyst, should be performed with proper planning and as soon as possible, avoiding injury to vital structures and possible occlusion sequelae.
References
1. Bocher L, Wonderberg Y, Ban-Zir J. Radiographic features of large cysts lesions of jaw in children. Paediatri Radiol. 2003;33:3-6. [ Links ]
2. Cardoso LC, Miyahara GI, Magro Filho O, Garcia Júnior IR, Soubhia AMP. Odontoma combinado associado a dentes não irrompidos: relato de casos clínicos. Rev Odont Araçatuba. 2003 Aug/ Dec;24(2):47-51.
3. Cildir SK, Sencift K, Olgac V, Sandalli N. Delayed eruption of a mandibular primary cuspid associated with compound odontoma. J Contemp Dent Pract. 2005;6:152-9.
4. Freitas DA, Freitas VA, Mol VC, Mana Neto L, Mol VC. Elemento dental impactado por odontoma composto. Rev Bras Cir Cabeça Pescoço. 2009 Jul/Aug/Sep;38(3):198-9.
5. Hisatomi M, Asaumi J, Konouchi H, Holanda Y, Wakasa T, Kish K. A case of complex odontoma associated with an impacted lower deciduos second molar and analysis of the 107 odontomas. Oral Dis. 2002;8:100-5.
6. Ikeshima A, Tamura Y. Differential diagnosis between dentigerous cyst and benign tumor with an embedded tooth. J Oral Sci. 2002;44:13-7.
7. Kaugars GE, Miller ME, Abbey LM. Odontomas. Oral Surg Oral Med Oral Pathol. 1989;67:172-6.
8. Lukes SM, Wachter KM. Compound odontoma: a case study. The Journal of a Dental Hygiene. 2003;77(1):47-9.
9. Mehra P, Singh H. Complex composite odontoma associated with impacted tooth. N Y State Dent J. 2007;73(2):38-40.
10. Motamedi MH, Talesh KT. Management of extensive dentigerous cysts. Br Dent J. 2005;198:203-6.
11. Morning P. Impacted teeth in relation to odontomas. Int J Oral Surg. 1980;9:81-91.
12. Nóia CF, Oliveira FAC, Pinto JMV, Santos WHM. Odontoma composto. RGO. 2008 Apr/ Jun;56(2):213-7.
13. Neville BW, Damm DD, Allen CM, Bouquot JE. Oral and maxillofacial pathology. 3. ed. St. Louis: Saunders Elsevier; 2009.
14. Santos TCRB, Sampaio RKPL. Aspectos clínicos, radiográficos e histopatológicos dos odontomas. Rev Bras Odontol. 1981;38(2):29- 36.
15. Serra-Serra G, Berini-Aytés L, Gay-Escoda C. Erupted odontomas: a report of three cases and review of the literature. Med Oral Patol Cir Bucal. 2009 Jun;14(6):299-303.
16. Silva LF, David L, Ribeiro D, Felino A. Odontomas: a clinicopathologic study in a portuguese population. Quintessence Int. 2009 Jan;40(1):61-72.
17. Smith JL, Kellman RM. Dentigerous cysts presenting as head and neck infections. Otolaryngol Head Neck Surg. 2005;133:715-7.
18. Tomizawa M, Otsuka Y, Noda T. Clinical observations of odontomas in Japanese children: 39 cases including one recurrent case. Int J Paediatr Dent. 2005;15(1):37-43.
19. Veis A, Tziafas D, Lambrianidis T. A case report of a compound odontoma causing delayed eruption of a central maxillary incisor: clinical and microscopic evaluation. J Endod. 2000;26(8):477-9.
 Corresponding author:
Corresponding author:
Yuri Edward de Souza Damasceno
Rua Travessa 1.ª de Queluz, n. 226
CEP 66090520 – Belém – PA – Brasil
E-mail: yuri.damasceno@hotmail.com
Received for publication: July 9, 2014
Accepted for publication: September 17, 2014
