










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRSBO (Online)
versão On-line ISSN 1984-5685
RSBO (Online) vol.12 no.3 Joinville Jul./Set. 2015
ORIGINAL RESEARCH ARTICLE
Assessment of oral health status of children with special needs in Delhi, India
Abhishek MehtaI; Radhika GuptaI; Saleha MansoobI; Shahnaz MansooriI
I Department of Public Health Dentistry, Faculty of Dentistry, Jamia Millia Islamia – New Delhi – India
ABSTRACT
Introduction: Children with special needs are considered to be a high risk group for dental diseases especially dental caries and periodontal diseases. Objective: Assessment of oral health status of children with special needs in Delhi, India. Material and methods: A cross sectional survey was conducted on 414 children with special needs belonging to four different disability groups i.e. Intellectually Disabled (ID), Physically Challenged, visually and hearing impaired. WHO Oral Health Assessment Form for children, 2013 was used for assessment of various parameters of oral health among the study population. Results: Of the 414 children, 305 were males and 109 females. Overall caries prevalence was 38%. Mean DMF value was 3.71 with ID children having higher mean than the other groups. A significant positive correlation was also observed between age and dental caries. Gingival condition was also worse in ID children and best in physically challenged ones. Highest numbers of trauma cases were recorded in visually impaired group. Delayed eruption of permanent teeth was most common in hearing impaired. 98.7% children required some form of dental treatment. Conclusion: Oral health of children with special needs was poor and urgent attention is required to plan a comprehensive dental health care programme for them.
Keywords: children with special needs; oral health assessment; intellectually disabled.
Introduction
The American Health Association defines a child with disability as a "child who for various reasons cannot fully make use of all his or her physical, mental and social abilities". According to WHO estimates, individuals with disability comprise 10% of the population in developed countries and 12% in developing countries 6. Census of year 2011 has revealed that over 26.8 million people in India as suffering from one or the other kind of disability. Among the total disabled in the country i.e. 26.8 million – 15 million are males and 11.8 million females. According to the census, 20.3% of the disabled are physically challenged followed by hearing impaired (18.9%) and visually impaired (18.8%). Nearly 5.6% of the disabled population is in ID group 7.
Oral health affects one's aesthetic and communication abilities; also it has strong biological, psychological, and social projections. People with disabilities deserve the same opportunities for oral health and hygiene as any other human being 1. Unfortunately oral health care is one of the greatest unattended health needs of the disabled people. Children with disabilities may have more marked oral pathologies, either because of their actual disability or for other medical, economic or social reasons, or even because their parents find it very difficult to carry out proper daily oral hygiene (e.g., cariogenic effect of medicines with high sugar content, excessive tooth grinding with self-mutilating behaviours) 13.
A higher prevalence and severity of oral diseases was observed by various investigators in disabled individuals around the World 1,3,10,19 and India 2,5,11,12,16,18. On the basis of these reports there are many unmet dental needs in disable population which need more attention. However, only limited studies have been done to compare dental health of different kinds of children with special needs 2,18. Majority of these studies have concentrated on one or two aspects of oral health while assessing oral health status of this group of children. A detail picture of oral health status of children with special needs is important when planning for a comprehensive dental programme for them as well as for lobbying efforts with health authorities. Keeping above facts in mind, an oral health survey was designed utilizing WHO oral health assessment form, 2013 21 which will provide us a full picture of oral health status of chi ldre n with special needs in the age range of 3-15 years attending various special schools in Delhi.
Material and methods
A cross sectional descriptive survey was conducted among 414 children of 3-15 years of age who are suffering from various kinds of disabilities and attending special needs schools in different parts of Delhi state in India.
Survey groups and sample size
There is no data available on number of children attending special schools in Delhi, therefore data from census of 2011 was utilized to find out total disabled population in Delhi state. The census states that total disabled population, includes all age groups, is less than 1.75% of total population of Delhi; in 0-6 year age group, 13,760 children are suffering from various disabilities 7, therefore by highest estimate possible and checking the data from previous census, the sample population will not be more than 50,000. Hence, the calculated sample size is 381 at 95% confidence interval, 80% power and expected frequency of dental caries at 50% (Statcalc, Epinfo version-7). The survey included 4 major disability groups as mentioned below with their sample size
i. Intellectually disabled (ID)=100;
ii. Visually impaired (VI)=90;
iii. Hearing impaired (HI)=132;
iv. Physically challenged (PC)=92.
Ethical clearance and informed consent
Informed consent was obtained from parent/ guardians and p ermission h ad be en taken from respective school authority prior to the clinical examination of children. Ethical clearance was obtained from the Ethical Research Committee of Jamia Millia Islamia University, New Delhi. In total eleven institutions located in various part of Delhi state were shortlisted for the study, out of these, nine institutions gave their consent to participate in the study.
Training and calibration of examiners
Clinical data was collected by three investigators under one main researcher. A recording clerk also assisted during the process. Before starting the main survey, a pilot study was conducted on 25 subjects of similar age group in the Out Patient Department of Public Health Dentistry for the purpose of training and calibration of examiners. Cohen's Kappa coefficient for assessment of dental caries was 0.82, indicating a good interexaminer reliability.
Inclusion and exclusion criteria
Children present on the day of examination were included in the study. A second visit was made to examine absentees. Those who are not willing to participate or unwell were excluded. Data was collected over a period of two months.
Data recording
Dental examinations were held in the respective schools under natural l ight with suf f icient illumination with participants seated in the ordinary chair. Examination was carried out using mouth mirror and Community Periodontal Index probe. Help of Teachers/care taker were utilized for communication with the children.
WHO Oral Health Assessment Form (2013) for children's was used for recording oral health status of the subjects. Information collected through this form included general information pertaining to study subjects like Name, Date of Birth, Age, and Gender. Clinical assessment includes recording of dentition status of child for caries and its effect like missing or filled teeth due to caries. Gingival status was assessed by recording gingival bleeding using CPI probe. Presence and severity of Dental erosion, Dental fluorosis and dental trauma were also been assessed.
A tooth was classified as missing if it had not erupted after six months of its expected eruption date. A tooth was classified as retained if it was still in the arch after six months of its expected date of exfoliation. Intervention urgency / treatment needs were also mentioned according to the type of treatment required for an individual.
After the examination children in need of dental treatment were referred to the faculty for rendering specialty care.
Statistical analysis
Data were analyzed using the Statistical Package for Social Sciences (SPSS), version 17 (IBM Software Company, USA). Epinfo version 7 was used for calculating the sample size. Frequency tables were prepared and mean and standard deviation were calculated. As the data was not following normal distribution, Mann Whitney U test was applied for pairwise comparison and Kruskal Wallis for comparing more than two variables. Pearson correlation test was used to check correlation between age and dental caries experience. Statistical significance was set at P ≤ 0.05.
Results
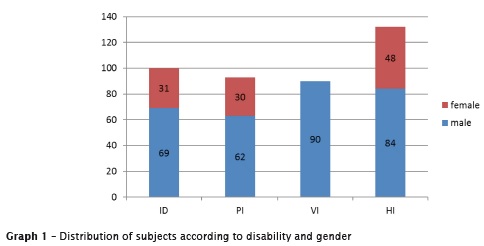
A total of 414 children comprised the sample, among them males were in overwhelmingly majority, representing 73.6% (305) of the total population (graph 1).
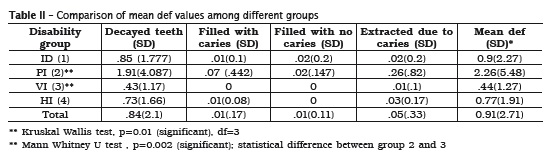
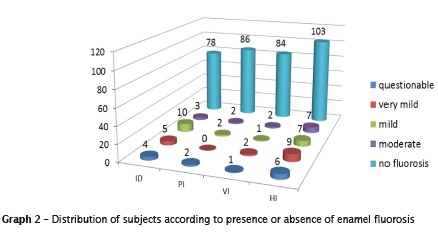
Mean Decayed Missing Filled Teeth (DMF) and Standard Deviation were calculated for various groups and are presented in table I. Overall comparison between groups using Kruskal-Wallis test showed that there was significant difference between the groups for dental caries experience in permanent dentition. When pairwise comparison was done using Mann Whitney test, it was found that dental caries experience was higher in intellectually disabled when compare to physically challenged group only, other comparisons were not significant. The largest component in DMFT was D component and F had very low values. In primary dentition, physically challenged children had significantly higher mean def values compared to visually impaired group (p<0.01) (table II). Overall caries prevalence was 38% in study population. A significant positive correlation was observed between age and dental caries (p<0.001, Pearson correlation test). Enamel fluorosis of different severity was present in 63 (15.2%) subjects. There was no case of severe fluorosis (graph 2).
Overall prevalence of dental trauma was 21%. Inter-group comparison was statistically significant and pairwise comparison showed that visually impaired were having highest cases of dental trauma in comparison to all the other groups (table III).
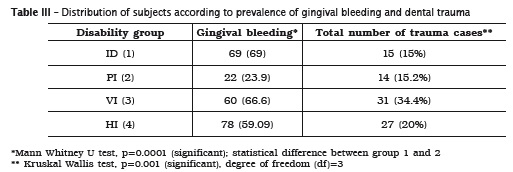
In total 55.3% of children was suffering from gingival bleeding. There was statistically significant difference between the groups with intellectually disabled children having higher gingival bleeding score. When pairwise comparison was done, intellectually disabled had statistically significant higher gingival bleeding score than Physically impaired group only and not significant with other two groups (table III).
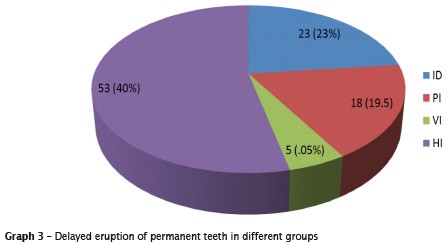
Pattern of delayed eruption of permanent teeth was also analyzed. In total 24% of children had delayed eruption of one or more teeth. Highest number was seen in hearing impaired children. (graph 3).
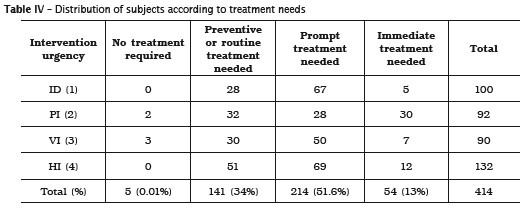
Only five children out of 414 did not require any form of dental treatment. Prompt dental treatment including scaling was required in 214 (51.6%) children, immediate treatment needed due to pain or infection due to dental/oral origin in 13% and preventive or routine treatment in 34% of the total sample population (table IV).
Discussion
Oral health is an integral part of general health and well being. Disabled people have equal right for good oral health as any other citizen of the country. Unfortunately due to their condition and lack of awareness towards oral health, dental diseases get undiagnosed in these children leading to accumulation of high unmet demand for dental care later in life.
A cross-sectional descriptive survey was conducted in various institutes opened for children with special needs in Delhi state, India. In total 414 children, 305 males and 109 females, from nine institutes were examined for various oral diseases and treatment needs. Due to this imbalance in gender number, no comparison was done of various parameters between males and females. One reason for such disparity in sex ratio could be due reluctance of parents to send girl child to special institutions in India.
Dental caries is a rapidly emerging oral health problem amongst the children of India. According to a National Oral Health Survey conducted in 2003-4, caries prevalence in India was 51.9, 53.8 and 63.1% at ages 5, 12 and 15 years, and mean DMF values were 2, 1.8 and 2.3 respectively 14. As per WHO Oral Health report (2003), mean DMF among 12 year children in Indian population was in range of 1.2-2.6 15.
The mean DMF value was 3.71 which is higher than as reported in above mentioned nationwide surveys, this means that although few children were suffering from dental caries, the severity of caries was higher in these children as compared to general population of children. Second explanation can be because of prior removal of carious teeth or due to periodontal reasons, especially among those with severe intellectual disabilities, living in institutional settings 9.
The mean DMF value in ID children was lower than various studies conducted around India 12,16. Similarly, visually and hearing impaired had slightly less mean DMF value as compared to studies done on special children in Bhopal 18, Delhi 5, Rajasthan 20 and comparable to that of Udaipur and Delhi 11,21.
In our study, overall caries prevalence was 38%. A partial explanation for low caries prevalence in comparison with general population may be that in many institutional and group settings, residents receive a well balanced diet, with supervised intake of refined carbohydrates 9.
A positive correlation of caries experience was observed with age, this finding is significant as it implies that burden of caries is going to increase in this population if necessary steps are not take immediately.
Various studies 2,17,20 and systematic review 4 have reported poorer oral hygiene especially among children with intellectual disabilities as compare to general population. In the current study, oral hygiene was assessed by presence or absence of gingival bleeding. Overall presence of gingival bleeding was 59.09%. Intellectually disabled had worst oral hygiene with 69.9% of them suffering from gingival bleeding. Physically impaired were having better gingival status among all the four groups. Similar results were obtained in study done by Shukla et al. 21.
Various reasons can be predicted for such finding like lack of intellectual abilities that precludes adequate oral hygiene practice. Individuals with problems of vision are able to comprehend oral hygiene instructions and also have more normal kinetic skills; however, they may still have difficulty seeing and removing plaque. Thus the most important variable in determining oral health status is the type of disability and how that disability impacts the maintenance of adequate or sound oral hygiene 17. Many different types of specially designed manual toothbrushes have been developed. Among them is the triple-headed brush, which is designed to clean the oral, buccal, and occlusal surfaces of the teeth with a single stroke and is recommended for certain individuals with limited manual skills 8.
Current study reported the highest incidence of dental trauma especially in maxillary incisors in visually impaired children; reason for this finding is obvious as this group has difficulty in seeing properly, hence they are more prone to accidents/fall.
Delayed eruption of teeth was seen in all groups but highest prevalence was observed among hearing impaired children. This finding requires further research.
Demand for dental treatment was quite high in these children as only five children did not require any dental treatment. This finding implies that all groups were deprived of dental care with very high unmet needs.
Among the limitations of the study are - utilization of convenience sampling technique, no attempt was being made to evaluate the severity of disabilities and level of motor skills of the study population and also the social and behavioral factors which are associated with oral health.
Conclusion
From the results, it can be concluded that oral health status of the children with special needs was poor with very low prevalence of treatment done and high unmet needs. The mean DMFT was significantly higher among ID and visually impaired individuals, whereas poor gingival condition and delayed eruption reported in hearing impaired individuals. Dental trauma was seen more in visually impaired children. The level of treatment or care by the society of its neglected and dependent part determines its cultural level and evolution. Children with special needs deserve special attention in the area of oral health as reflected in this study.
Acknowledgements
We are thankful to ICMR-STS programme for the approval of this project and to all the students and head of institution of special schools who participated in this study.
References
1. Altun C, Guven G, Akgun OM, Akkurt MD, Basak F, Akbulut E. oral health status of disabled individuals attending special schools. Eur J Dent. 2010 Oct; 4(4):361-6. [ Links ]
2. Ameer N, Palaparthi R, Neerudu M, Palakuru SK, Singam HR, Durvasula S. Oral hygiene and periodontal status of teenagers with special needs in the district of Nalgonda, India. J Indian Soc Periodontol. 2012;16:421-5.
3. Anaise JZ. Periodontal disease and oral hygiene in a group of blind and sighted Israeli teenagers 14- 17 years of age. Community Dent Oral Epidemiol. 1979;7:353-6.
4. Andres Al, Davis EL. Oral health of patients with intellectual disabilities: a systematic review. Spec Care Dentist. 2010;30(3):110-7.
5. Avasti K, Bansal K, Mittal M, Marwaha M. Oral health status among sensory impaired children in Delhi and Gurgoan. International Journal of Dental Clinics. 2011:3(2):21-3.
6. Baykan Z. Causes and prevention of disabilities, handicaps, and defects. J Cont Med Educ. 2003;9:336-8.
7. Census of India 2011. Data on Disability. Available from: URL:http://www.censusindia.gov. in.
8. Dogan C, Alacam A, Asici N. Clinical evaluation of the plaque removing ability of three different toothbrushes in a mentally disabled group. Acta Odontol Scand. 2004;62;350-4.
9. Gabre P, Martinsson T, Gahnberg L. Incidence of, and reasons for, tooth mortality among mentally retarded adults during a 10-year period. Acta Odontol Scand. 1999;57:55-61.
10. Hashemi Z, Hajizamani A, Bozorgmehr E, Omrani F. Oral health status of a sample of disabled population in Iran. J Oral Health Epidemiol. 2012;1(1):23-8.
11. Jain M, Mathur A, Kumar S, Dagli RJ, Duraiswamy P, Kulkarni S. Dentition status and treatment needs among children with impaired hearing attending a special school for deaf and mute in Udaipur, India. J oral Science. 2008;50(2):161-5.
12. Jain M, Mathur A, Sawla L, Choudhary G, Kabra K, Duraiswamy P et al. Oral health status of mentally disabled subjects in India. Journal of Oral Science. 2009;51(3):333-40.
13. McPherson M, Arango P, Fox H. A new definition of children with special health care needs. Pediatrics. 1998;102:137-40.
14. National Oral Health Survey and Fluoride mapping of India. Dental Council of India 2002- 2003.
15. Petersen PE. The World Oral Health Report 2003: continuous improvement of oral health in the 21st century – the approach of the WHO Global Oral Health Programme. Community Dent Oral Epidemiol. 2003;31(Suppl 1):3-23.
16. Purohit BM, Acharya S, Bhat M. Oral health status and treatment needs of children attending special schools in South India: a comparative study. Spec Care Dentist. 2010;30:235-41.
17. Rao D, Amitha H, Munshi AK. Oral hygiene status of disabled children and adolescents attending special schools of South Canara, India. Hong Kong Dent J. 2005;2(2):107-13.
18. Reddy VK, Chaurasia K, Bhambal A, Moon N, Reddy EK. A comparison of oral hygiene status and dental caries experience among institutionalized visually impaired and hearing impaired children of age between 7 and 17 years in central India. J Indian Soc Pedod Prev Dent. 2013;31:141-5.
19. Shaw L, Maclaurin ET, Foster TD. Dental study of handicapped children attending special schools in Birmingham, UK. Community Dent Oral Epidemiol. 1986;14:24-7.
20. Singh A, Kumar A, Berwal V, Kaur M. Comparative study of oral hygiene status in blind and deaf children of Rajasthan. J Adv Med Dent Sci. 2014;2(1):26-31.
21. Shukla D, Bablani D, Chowdhry A, Zafri Z, Ahmed N, Mishra S. Oral health status and dental caries experience in mental l y challenged individuals. Ann Public Health Res. 2014;1(2):1008-12.
22. World Health Organization. Oral health surveys-basic methods. 5. ed. Geneva: WHO; 2013.
 Corresponding author:
Corresponding author:
Abhishek Mehta Department of Public Health Dentistry
Faculty of Dentistry
Jamia Millia Islamia
New Delhi – India
E-mail: mehta_abhishek2003@yahoo.co.in
Received for publication: July 27, 2015
Accepted for publication: August 12, 2015
