










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRSBO (Online)
versão On-line ISSN 1984-5685
RSBO (Online) vol.12 no.3 Joinville Jul./Set. 2015
ORIGINAL RESEARCH ARTICLE
Accuracy of Root ZX mini and Raypex 6 in locating the apical foramen of molars: radiographic and microscopic evaluation
Berenice R. García-HerverthI; Norberto J. BroonII; Alvaro CruzIII; Claudia A. Palafox-SánchezIV; Santiago Andaracua GV; Ricardo Ayón-GarcíaVI
I Endodontic Specialist, Military School of Sanidad Graduates, University of Army and Air Forces – Mexico, D.F.
II Private practice in Endodontics. Health Sciences University Center, University of Guadalajara – Guadalajara – Mexico
III Biomedical Sciences Investigation Institute, Professor in the Endodontics program of the Health Sciences University Centre, University of Guadalajara – Guadalajara – Mexico
IV Biomedical Sciences Investigation Institute, Professor in the Biomedical Sciences Postgraduate program and in the Endodontics program at the Health Sciences University Centre, University of Guadalajara – Guadalajara – Mexico
V Private practice in Endodontics. Autonomus University of Queretaro – Queretaro – Mexico
VI Student in the Endodontics program at the Health Sciences University Centre, University of Guadalajara – Guadalajara – Mexico
ABSTRACT
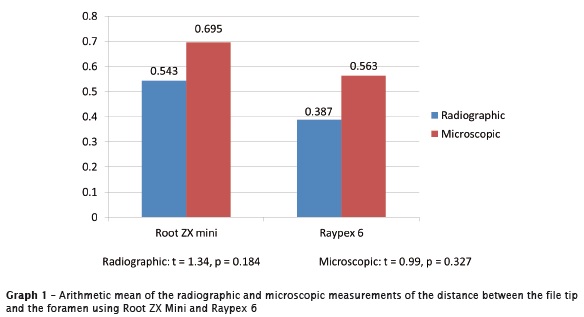
Introduction: The precise localization of the apical foramen and the odontometry determination is an important stage since it locates the apical limit for instrumentation and filling. Objective: To compare the accuracy of Root-ZX Mini and Raypex 6 in locating apical foramen in extracted molars. Material and methods: 80 mesial and buccal canals from 40 mandibular and maxillary human molars were used. A size #15 K-file was introduced to canal, until the locator indicated the apical foramen (red bar/line in both devices). With the file in position, it was re-adjusted for Root-ZX II Mini on the green bar and on the two yellow bars for Raypex 6. All the samples were measured from the tip of the file to the apical foramen with radiovisiograph and the Sidexis software. The apical third of the root was shaved until exposure of the file. The distance from the file tip to the most coronal border of the apical foramen was obtained and it was measured with a clinical microscope at 16-fold magnification. The measured lengths with the radiovisiograph and the clinical microscope were analyzed with the statistical Student's T-test. Results: The average length from the tip of the file to the apical foramen using Root-ZX Mini was 0.695 mm and 0.543 mm with Raypex 6. There was no significant difference. Conclusion: Two devices were accurate in locating apical foramen with an adequate level of reliability.
Keywords: apical locator; odontometry; working length.
Introduction
In endodontic treatment, the precise localization of the apical foramen and the working length determination is an important stage since it locates the apical limit for instrumentation and filling 22. The location aims to endodontic procedures are performed within the anatomic limits of the root canal 18.
The radiographic technique has been used to determine the working length, however, it shows diverse clinical limitations: it has a subjective interpretation; there is overlapping of anatomic structures; there may be image distortion; it is difficult to determine the position of the apical foramen; the quality of the film or of the sensor may affect the image; it´s a bi-dimensional image of a three-dimensional object. In addition, some clinical circumstances limit its use, such as patients with macroglossia, nausea, pediatric patients or pregnant women 9.
The electronic method to locate the apical foramen was firstly introduced by Custer 4 in 1918, using the electrical conductivity principle 9. In 1942, Susuki 24 indicated that the electrical resistance between an instrument inserted inside the root canal and an electrode adhered to the oral mucosa, registered constant values 11,13. Based on this principle, Sunada 23 developed a simple direct-current device to measure the canal length. Later, equipment that employed impedance at simple or multiple frequencies were designed, which have overcome some observed problems in the first models and they have been overcoming the problems that the first devices had 8. The fourth generation apparatus employed two separate frequencies (400 Hz and 8 kHz), and measured the resistance of two frequencies of alternating current at the same time, obtaining in this way the impedance ratio 9.
These locators are not affected by the presence of irrigants inside the canal, nevertheless, some inaccurate measurements are due to morphological (lateral, accessor y and convergent canals, bifurcations, resorptions and perforations) and technical aspects (contact with metals) 2.
To determine the working length, it is advisable to combine the use of periapical radiography and electronic apex locator 1,9,16,26. However, in clinical situations with difficulty to obtain the working length with periapical radiograph 6, only the electronic device is used.
The release of new models of devices for electronic working length requires their assessment to allow the verification of their reliability. Thus, the purpose of this study is to compare the accuracy in locating of the apical foramen in mesial and buccal canals of extracted molars, using Root ZX Mini and Raypex 6, with radiographic and microscopic evaluation.
Material and methods
Eighty mesial and buccal canals from forty mandibular and maxillary human molars were used with approval of the Bioethics Committee of the Military Hospital. They were obtained from the Maxillofacial Surgery Service from the Dental Specialist Centre of the Mexican Army and Air Force, México. The Root ZX Mini (JJ Morita, Tokyo-Japan) and Raypex 6 (VDW, Munich-Germany) devices were used, dividing the samples in two study groups of 40 canals each, the electronic measurements were made with both devices.
With a diamond disc (SS White – USA) the clinical crown was cut off from all the pieces at the cementum-enamel junction; they were individualized into mesial or buccal roots, sectioning the roots in cross direction to the longitudinal axis to obtain a flat border with the teeth root axis, achieving in this way direct vision to the root canal.
The canals were located with the DG16 (SS White – USA) explorer and they were negotiated with #15 or 10 K file (Dentsply-Maillefer, Ballaigues – Switzerland). The entrance to the canals was irrigated with a 5 ml of 5.25% sodium hypochlorite (NaOCl) (Viarzonit T – México, D.F.) and the canals orifices were enlarged with #4 Gates-Glidden drills (Dentsply-Maillefer Ballaigues – Switzerland). The pulp chamber was flooded with NaOCl.
The roots were positioned vertically in a vegetal sponge wetted with a 3 ml. 0.9% Sodium Chloride solution (Kabipac – Mexico, D.F.), the sponge was placed in a glass container, simulating the natural oral humidity. The manufacturer's recommendations were followed for both devices.
The electrode was placed in contact with the humidity of the sponge to complete its circuit. A size #15 K file (Dentsply-Maillefer, Ballaigues – Switzerland) was inserted in the root canal until the apical foramen was felt. The file-holder was placed at the stem of the instrument and the position of the file inside the apical foramen was confirmed with either one or the other electronic device (the red bar was illuminated). The working length was re-adjusted. In the case of the Root ZX Mini, it was on the green bar and with the Raypex 6 in the first two yellow bars (both devices at 0.5 mm). The lecture was left to stabilization for 5 seconds. Then the file-holder was removed from the number 15 K file and it was fixed to the root dentin with cyanoacrylate adhesive (Kola-loka, Mexico) and light-cured resin (3M ESPE, Germany), verifying the reading again in the foramen locator.
Digital radiographs were taken with collimator (Dentsply-Mexico) using the parallelism technique; a phosphorus film scanner "Vista Scan Dürp Dental" (Henry-Schein – México, D.F.) was used on all the samples, on to which was previously placed a scaled template.
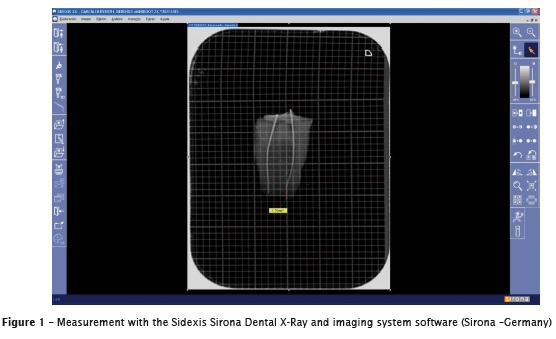
The measurements were done by two operators in the digital radiography, using the Radiovisiograph (Sirona-Germany) and the Sidexis Sirona Dental X-Ray software (Sirona-Germany). The pointer was positioned from the file tip (initial point) and a line was drawn towards the apical radiographic apex (figure 1), registering the distance in millimeters in a data-collection sheet.
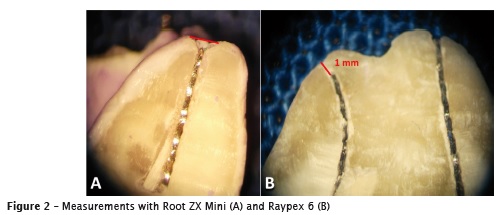
With the use of the clinical microscope Ompi 99 (Zeiss, Germany) at 16-fold magnification and a fine-grain conical diamond bur (SS White, México) at high speed the 4 apical millimeters were trimmed in longitudinal direction until the file was exposed. Pictures were taken (figure 2) using the clinical microscope OPMI 1 FR pro (Zeiss-Mexico) at 16-fold magnification and a digital camera (Sony-Japan).
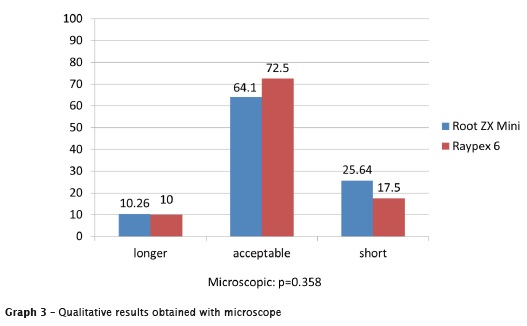
To perform the microscopic measurements, 2 calibrated examiners used Corel-Draw 4 software. In the first place, the CDJ zone and the apical foramen were identified. A line from the mesial to the distal wall was drawn on both anatomical zones. The intersection of the straight line coming from the tip of the file towards the center of the apical foramen was considered as the measuring point. These results were grouped in three categories, according to Piasecki et al. 15. All the values were registered in a data-collection sheet and were analyzed with the Student's T-test, with a significance level of 0.05.
Results
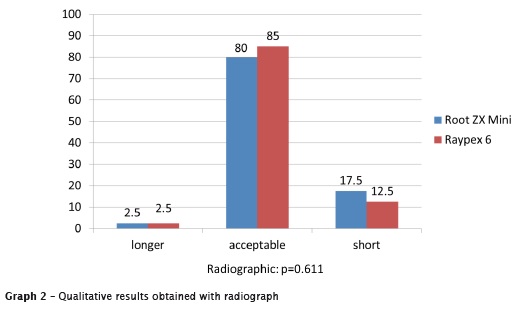
The radiographic and microscopic measurements results are shown in the graph 1. The results grouped in the 3 qualitative results: long, acceptable, and short are shown in graph 2 and 3. No significant difference was observed between both electronic devices, in all of the evaluating methods.
Discussion
The major canal is apically limited by the apical foramen. The pulp and periodontal tissues converge at the CDJ (cement dentin junction), located on average 1 to 2 mm from the apical foramen 9. However, it is not possible to determine the exact position of the CDJ using radiographs in a precise way 12,15, moreover, this joint of cement and dentin may be present at different heights in the same canal, depending on the observed wall; thus, it also could be referred as CDJ zone and not CDJ limit. This CDJ zone is located on average 1 to 1.5 mm from the apical radiographic apex, but this length may vary 9.
The precision of the electronic devices is based on the fact that the double-frequency devices possess a calibration that allows the indication of the variation of impedance relative values (quotient or difference) from the apical region, permitting the location of the instrument tip near 1 mm of the apical foramen, which is near to the apical constriction 9. This position was proved when the ability of Root ZX to detect the presence of the apical constriction in teeth, with or without foramen patency, was tested. The analysis of the impedance values showed that the equipment was actually based on the detection of the decrease in the dentin thickness in the apical third of the root canal 9.
The electronic method yields similar results as the radiographic one 16,17,25, regarding to the apical foramen localization. Nevertheless, the electronic devices have the advantage that their reference point is the apical foramen, which is imperceptible in the radiographs 12. The radiographic method has as reference point, the radiographic apical apex, which in the majority of cases differs in the location of the major foramen 19.
The precision was evaluated of three electronic foramen locators and compared them with the digital radiograph 1. They observed that there was no significant difference between the two examined radiographic planes in comparison with the electronic measurements. In the present study, it was observed an interval from 0.543 mm to 0.387 mm between the precision of the radiographic location of the foramen with both devices, which in the clinical practice will allow locating the CDJ zone. The localization of the foramen is clinically acceptable, with a ±1 mm margin from the CDJ zone, however, the ±0.5 mm margin to the minor diameter of the CDJ zone is acceptable 7,15,20.
The accuracy of locating the apical foramen of the Root ZX and Novapex also was evaluated with a ±0.5 mm tolerance 3. They observed the foramen location between 82% (Novapex) and 89% (Root ZX) with no statistical difference between them. With a margin of ±1 mm. MiniApex locator and Raypex 5 was evaluated and obtained a precision of 100%, whereas with the margin of ±0.5 mm, the two devices had the 75% of accuracy, with no statistical difference between them 21. With the same measuring range were evaluated ex vivo the reading accuracy of Root ZX, Bingo 1020 and Ipex in respect to the real measure of the teeth. They concluded that all electronic devices tested were able in determining the precise tooth length when considered a variation of 1 mm from the position of apical foramen 10. Root ZX, Raypex 5 and the Elements Apex locator regarding to their precision to detect the minor foramen and the morphological factors that inf luence the determination of the working length 5. They point out that the minor foramen morphology and the major foramen location are influencing factors on the measurements by the apical locators. Another factor that they may interfere on the location of the foramen is the presence of apical resorption in teeth with apical periodontitis, however, Root ZX showed precision for the location of the apical foramen in the presence of apical periodontitis 15. Elsewhere Root ZX II and Propex II were compared to establishment working length and direct visual measurement. Both apex locators showed an acceptable percentage of correct readings 14. In the present study, recently extracted teeth were used, without considering if apical resorption existed or not. In this study both electronic locators, Root ZX Mini and Raypex 6, showed reliability for the determination of the apical foramen, showing precision in ±1 mm with no statistical difference between them.
Conclusion
Under the ex vivo conditions in this study, Root ZX Mini and Raypex 6 were precise in locating the apical foramen in mesial canals of lower molar and buccal canals of upper molar teeth, with the same reliability as the digital radiographs of the extracted roots. It is recommended to perform in vivo clinical studies with these devices, to consider all the variables present in clinic.
Acknowledgements
To Dr. Luis Gerardo Gascón Guerra for facilitating the use of the clinical microscope of the post graduation program in Endodontics from the Health Sciences University Centre, University of Guadalajara, Mexico. To Drs. Carlos Guerrero Bobadilla and Gustavo Martin del Campo Plascencia for teaching the clinical use of microscope from the Health Sciences University Centre, University of Guadalajara, México.
References
1. Cianconi L, Angotti V, Felici R, Conte G, Mancini M. Accuracy of three electronic apex locators compared with digital radiography: an ex vivo Study. J Endod. 2010;36:2003-7. [ Links ]
2. Cruz GA, Rojas JV, Rosano AL. Endodoncia: Fundamentos científicos para la práctica clínica. Guadalajara: Amate Editorial; 2012. p. 103-46.
3. Cunba FL, Albuquerque DS, Correia L. The ability of two apex locators to locate the apical foramen: an in vitro study. J Endod. 2006;32: 560-2.
4. Custer LE. Exact methods of locating the apical foramen. J Natl Dent Assoc. 1918;5:815-9.
5. Ding J, Gutmann JL, Fan B, Lu Y, Chen H. Investigation of apex locators and related morphological factors. J Endod. 2010; 36:1399- 403.
6. Dummer PHM, McGinn JH, Ress DG. The position and topography of the apical canal constriction and apical foramen. Int Endod J. 1984;17:192-8.
7. Duran-Sindreu F, Stöber E, Mercadé M, Vera J, Garcia M, Bueno R et al. Comparison of in vivo and in vitro readings when testing the accuracy of the Root ZX apex locator. J Endod. 2012;38:236-9.
8. Fan W, Fan B, Gutmann JL, Bian Z, Fan MW. Evaluation of the accuracy of three apex locators using glass tubules. Int Endod J. 2006;39:127-35.
9. Gordon MPJ, Chandler NP. Electronic apex locators. Int Endod J. 2004;37:425-37.
10. Heidemann R, Vailati F, Teixeira CS, Oliveira CAP, Pasternak Junior B. Análise comparativa ex vivo da eficiência na odontometria de três localizadores apicais eletrônicos: Root ZX, Bingo 1020 e Ipex. RSBO. 2009;6:8-12.
11. Hembrough JH, Weine FS, Pisano JV, Eskoz N. Accuracy of an electronic apex locator: a clinical evaluation in maxillary molars. J Endod. 1993;19:242-6.
12. Jakobson SJM, Westphalen VPD, Neto UXS, Fariniuk LF, Picoli F, Carneiro E. The accuracy in the control of the apical extent of rotary canal instrumentation using Root ZX and protaper instruments: an in vivo study. J Endod. 2008;34:1342-5.
13. Jenkins JA, Walker WA, Schindler WG, Flores CM. An in vitro evaluation of the accuracy of the Root ZX in the presence of various irrigants. J Endod. 2001; 27:209-11.
14. Miguita KB, Cunha RS, Davini F, Fontana CE, Bueno CES. Comparative analysis of two electronic apex locators in working length determination at endodontic therapy: an in vitro study. RSBO. 2011;8:27-32.
15. Piasecki L, Carneiro E, Fariniuk LF, Westphalen VPD, Fiorentin MA, Silva Neto UX. Accuracy of Root ZX II in locating foramen in teeth with apical periodontitis: an in vivo study. J Endod. 2011;37:1213-6.
16. Ravanshad S, Alireza A, Anvar J. Effect of working length measurement by electronic apex locator or radiography on the accuracy of working final length: a randomized clinical trial. J Endod. 2010;36:1753-6.
17. Renner D, Grazziotin-Soares R, Gavini G, Barletta FB. Influence of pulp conditions on the accuracy of an electronic foramen locator in posterior teeth: an in vivo study. Braz Oral Res. 2012;26:106-11.
18. Ricucci D, Langeland K. Apical limit of root canal instrumentation and obturation, part 2. A histological study. International Endodontic Journal. 1998;31:394-409.
19. Saito T, Yamashita Y. Electronic determination of root canal length by newly developed measuring device. Influences of the diameter of apical foramen, the size of k-file and root canal irrigants. Dent Japan. 1990;27:65-72.
20. Somma F, Castagnola R, Lajolo C, Holtzman LP, Marigo L. In vivo accuracy of three electronic root canal length measurement devices: Dentaport ZX, Raypex 5 and Propex II. Int Endod J. 2012;45:552-6.
21. Stöber EK, de Ribot J, Mercadé M, Vera J, Bueno R, Roig M et al. Evaluation of the Raypex 5 and the mini apex locator: an in vivo study. J Endod. 2011;37:1349-52.
22. Stoll R, Klein UB. Effectiveness of four electronic apex locators to determine distance from the apical foramen. Int Endod J. 2010;43:808-17.
23. Sunada I. New method for measuring the length of the root canal. J Dent Res. 1962;41:375-87.
24. Suzuki K. Experimental study of iontoforesis. Japanese J Stomatol. 1942;16:411-29.
25. Williams CB, Joyce AP, Roberts S. A comparison between in vivo radiographic working length determination and measurement after extraccion. J Endod. 2006;32:624-7.
26. Wrbas KT, Ziegler AA, Altenburger MJ, Schirrmeister JF. In vivo comparison of working length determination with two electronic apex locators. Int Endod J. 2007;40:133-8.
 Corresponding author:
Corresponding author:
Alvaro Cruz
Av. Francisco Javier Gamboa, n. 230, Col. Arcos Sur
CP 44150 – Guadalajara – Jalisco – México
E-mail: endoacruz@yahoo.com
E-mail: endobr1@hotmail.com
Received for publication: December 2, 2014
Accepted for publication: September 14, 2015
