










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRSBO (Online)
versão On-line ISSN 1984-5685
RSBO (Online) vol.12 no.3 Joinville Jul./Set. 2015
ORIGINAL RESEARCH ARTICLE
Resistance to fracture evaluation of endodontically treated roots of first maxillary premolars
Rosany Laurentina Santos de CarvalhoI; Carolina dos Santos GuimaraesI; Marcia Maria Fonseca da SilveiraI; Diana Santana de AlbuquerqueI; Raquel Azevedo de MoraesI; Flávia de Lima Cavalcanti SpinelliI
I Department of Dentistry, University of Pernambuco – Camaragibe/Recife – PE – Brazil.
ABSTRACT
Introduction:One of the most common dental procedures associated to vertical root fractures is the endodontic treatment with excessive dentin wall wear and another increasing risk factor is the use of intraradicular post. Objective: This study evaluated the resistance to fracture of the buccal and palatal roots of maxillary first premolars with endodontically treated canals and spaces for posts. Material and methods: Twenty two first permanent premolar roots (11 buccal and 11 palatal) composed the experimental sample. The canals were prepared with Protaper Universal® system until file F3 and then filled with gutta-percha cone F3 and endodontic sealer and received spaces for posts keeping 4 mm of filling at the apical third. The roots were subjected to compression test in a universal testing machine (Kratus). The roots were subjected to a progressive compression stress at a speed of 0.5 mm / min. A load cell of 200 kg was used. Results: Statistical analysis revealed significant differences between the strength values and resistance limit between groups (P<0.05), as analyzed by t Student test. The values of resistance to fracture of 0.44 kgf/mm2 for group 1 (buccal roots) and 0.31 kgf/mm2 for group 2 (palatal roots) were found. Conclusion: The resistance to fracture of the buccal roots was higher than that of palatal roots of first premolars submitted to biomechanical preparation and root preparation for intraradicular post.
Keywords: Endodontics; fracture compression; dental fissures; tooth fractures.
Introduction
The root fractures are injuries that cause damage to the mineralized tissues, periodontal ligament, and pulp and are classified into vertical, horizontal, and oblique and may occur in the cervical, medium, or apical third 7,16.
The dental procedure that is most commonly associated as a cause of vertical root fracture (VRF) is the endodontic treatment with excessive wear of dentin walls and the use of intracanal posts. This situation combined with the age of the patient may increase susceptibility to root fracture. The mandibular molars and maxillary premolars are the most affected teeth 3,5,13,18,21.
VRF is a condition difficult to diagnosis and repair, often resulting in failed attempts of endodontic retreatment. The anatomical characteristics and the mesial-distal flatness of the root of some teeth have been identified as the main predisposing factors for this fracture type, increased when the need for reconstruction by intraradicular post. In order to minimize this risk the dentist should select the root of higher strength with the easiest post placement, which should follow the shape of the selected root 15,20.
This study aimed to evaluate the fracture strength of the buccal and palatal roots of maxillary first premolars treated endodontically and with spaces made for post, for through compression tests in universal testing machine.
Material and methods
The study was approved by the Ethical Committee in Research of the University of Pernambuco (CEP / UPE) under the protocol CAAE: 13092913.3.0000.5207, and developed at the Laboratory of Mechanical Tests in Pernambuco Dental School, University of Pernambuco (FOP / UPE). This is a laboratorial in vitro study.
The sample comprised 22 roots of the maxillary first premolars, newly-extracted for therapeutic reasons, which on visual inspection showed straight roots and formed apex. Teeth, after the initial cleaning, were placed in 0.5% sodium hypochlorite, sterilized, and kept in distilled water under cooling, according to the protocol of the Bank of Teeth of BDH / FOUSP 14.
The teeth were radiographed to check the absence of calcifications or anatomical variations, inspected with an optical microscope (Callmex model – Q705M, Florianópolis, SC, Brazil), at x10 magnification, to observe the integrity of the roots. Both the crown opening and access to the root canal were executed with the aid of spherical diamond burs at high speed (KG Sorensen, São Paulo, SP, Brazil), according to the pulp chamber size, and Endo – Z burs (KG Sorensen, São Paulo, SP, Brasil), to remove pulp ceiling. The teeth were sectioned vertically, with double-sided diamond disc (KG Sorensen, São Paulo, SP, Brazil), at the furcation, separating the buccal and palatal roots. The roots were divided into two groups: group I (11 buccal roots) and group II (11 palatal roots).
The working length of the roots was determined by the visual method by introducing a size 15 file (Flexofile, Dentstply, Maillefer, Switzerland), inside the root canal until it reaches the foramen, then backing up a millimeter. The channels were prepared using the Protaper Universal® system (Dentsply Maillefer – Ballaigues-Switzerland) and X-Smart® motor (Dentsply Maillefer – Ballaigues-Switzerland), set up in 250 rpm rotation and 3N torque, always under irrigation with 1.0% sodium hypochlorite (Fórmula & Ação – São Paulo, Brazil). The canals were filled with gutta-percha point size F3 and AH Plus sealer. Then the spaces for the posts were made with the aid of Gates Glidden drills size #3, keeping 4 mm at apical third. Next, the roots were wrapped in a sheet of lead and Vaseline were applied on the samples centralized in rings of polyvinylchloride (PVC) measuring 25x10 mm, closed at its base with utility wax no. #7, filled up to the cementumenamel limit with chemically activated acrylic resin (Art. Odontológicos Clássico Ltda., São Paulo, SP), creating an artificial socket. The lead sheet was removed from each tooth and a polyester-based molding material of high viscosity was inserted into the artificial socket with the aid of spatula no. #24, to mimic the periodontal ligament (Figure 1).

The teeth were stabilized and subjected to compression test on a universal testing machine (Kratos Equipamentos Industriais / model IKCL3 – USB), through a metal device with a tapered finger spreader D, 25 mm (Maillefer Dentsply), adapted on its upper end, allowing the force applied inside the canal was perpendicular to the long axis of the tooth (Figure 2).

The teeth were subjected to a progressive compressive force with a load of 200 at 0.5 kg mm/min. The vertical pressure was maintained until fracture, which was perceived by the sudden change of the chart on the computer screen. A chart was generated for each sample tested, and the values of resistance to fracture forces were submitted to statistical test for comparison between the experimental groups.
The study evaluated the resistance to fracture of the buccal and palatal roots of the maxillary first premolar by using a laboratory method (compression test).
The statistical program used for data entry and statistical calculations was Statistical Package for Social Sciences version 21 (SPSS). Statistical significance was set at p<0.05 and confidence interval were determined at the level of 95%.
Data regarding to the average basic measures, standard deviations, and variation coefficients were analyzed by Student's t test.
Results
Statistical analyzes of the strength values and tensile strength, as shown in Table I, evidencing the comparison between the groups exhibited a statistically significant difference (P<0.05).
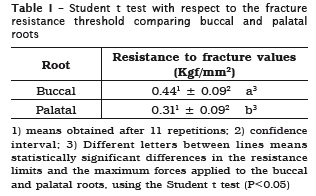
The resistance to fracture values were 0.44 Kgf/ mm2 for group I (buccal roots) and 0.31 Kgf/mm2 for group II (palatal roots). Thus, one can say with 95% confidence interval that there are significant differences between the resistance to fracture of the buccal roots when compared to palatal roots of teeth with root canal and post.
Discussion
Vertical root fractures can occur both in vital and devitalized teeth endodontically treated or not. The highest prevalence is related endodontically treated teeth. The literature confirms this statement 11,19,21, identifying as causes, most often, iatrogenic factors, as poorly-constructed intraradicular post and core, inadequate selection of teeth as fixed prosthesis abutments, poorly conducted endodontic treatment using excessive force to the spacer during the filling of the root canal system of through the lateral condensation technique.
The clinical decision-making regarding the best material and technique for reconstruction of teeth with severe coronary destruction should consider variables related to the patient (occlusion, masticatory force, level of alveolar bone, parafunctional habits) and variables related to the tooth morphology (length and volume of roots), to maximize the longterm prognosis of teeth endodontically treated and prepared for intraradicular post and core.
The first premolar has commonly two roots, and root variations consist of fused roots with separate canals, roots fused and linked or "tangles", roots fused with a common apical foramen and possibly teeth with three roots or two roots with three canals 17. In this study, we selected roots anatomically individualized, with similar length and root diameter in order to standardize the samples and reduce the possibility of misinterpretation regarding the best choice of position for cementation of intraradicular post and core 8.
It is always controversial determining which root is more appropriate to anchor to intraradicular post and core in endodontic treatments with prosthetic reconstruction of the first premolars with two roots. There is debate about the risk of fracture and the need for anchoring in one or both roots.
The anatomy of the root canal and is crucial to the success in placing intraradicular ´posts and the root preparation should be as the most conservative way as possible, especially in teeth with anatomical mesial-distal flattening 2,22.
In the case of the maxillary first premolars, the prevalence of two canals is around 95% in separate or fused roots, which result into a strong mesialdistal flattening at the cervical and middle thirds. The deep knowledge of tooth morphology, proper radiographic analysis, and aid of magnification, complemented with good lighting, decrease the occurrence of iatrogeny due to excessive wear of the remaining root and help in choosing the most appropriate root to anchor the post when the teeth require prosthetic reconstruction12.
The present study was designed to determine which root would be the most suitable to receive the intraradicular post in endodontically-treated maxillary first premolar subjected to compressive loads. The compression models have been adopted in the literature to evaluate the resistance to fracture of the various tooth types with biomechanical preparation and intracanal posts 1,7,10. However, they have not been used in the resistance to VRF analysis comparing the same tooth type, as performed in this study.
One clinical scenario was simulated in this study with an artificial periodontal ligament using a molding material to coat the root, which has a modulus of elasticity very similar to natural periodontal ligament 4.
The posts were not made after preparation of intracanal space to eliminate the parameters such as the material's structure, shape, length, and thickness of the posts. Thus, only the structural integrity and resistance to fracture of the root remnant after the post preparation was be tested more precisely 6.
The applicat ion of compressive force in endodont ically treated teeth is a method of resistance to fracture evaluation with a high degree of clinical relevance, since it can simulate conditions for applying forces similar to those of clinical conditions. The mean values of kg force needed to fracture these specimens were approximately 2.20 kgf for buccal roots and 1.56 kgf for palatal roots. Similar research conducted by Lertchirakarn et al.11 also calculated the safe load limit required to avoid VRF in several teeth. Six groups of ten teeth were tested: central incisors, premolars and upper and lower molars. The average fracture load was variable, with the upper incisors requiring higher load (17.2. kg) and the lower incisors lower load (6.2 kg). The results suggest that only the lateral condensation should not be the direct cause of VRF and situations where most wear occurs for the placement of intracanal post probably increases this risk, corroborating this study results, where all the tested specimens received intracanal post preparation, thereby increasing the wear of dentin walls 9,11.
Conclusion
The results of this study indicate greater resistance to fracture of buccal root than the palatal root of maxillary premolars filled and with preparation for intraradicular post and core. Anatomical aspects as volume and direction of the root canal should support the choice of the root to receive the post and core.
References
1. Al-Wahadni AM, Hamdan S, Al-Omiri M, Hammad MM, Hatamleh MM. Fracture resistance of teeth restored with different post systems: in vitro study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008 Aug;106(2):e77-83. [ Links ]
2. Bellucci C, Perrini N. A study on the thickness of radicular dentine and cementum in anterior and premolar teeth. Int Endodont J. 2002;35(7): 594-606.
3. Cohen, Berman LH, Blanco L, Bakland L, Kim JS. A demographic analysis of vertical root fractures. J. Endod. 2006 Dec;32(12):1160-3.
4. Coolidge ED. The thickness of the human per iodontal l igament . J Am Dent Assoc. 1937;24:1260.
5. Dekon S, Zavanelli A, Resende C, Paulo R, Neves R. Alternativas clínicas para confecção de núcleos protéticos estéticos. Rev Bras Prót Clín Lab. 2002;4(21):387-91.
6. Dilmener FT, Sipahi C, Dalkiz M. Resistance of three new esthetic post- and-core systems to compressive loading. J Prosthet Dent. 2006 Feb;95:130-6.
7. Garcia LFM, Caldeira, CL. Vertical fracture resistance of endodontically treated teeth with different root filling materials. Rev Odontol Univ Cid São Paulo. 2010 May-Aug;22(2):104-10.
8. Hegde J, Ramakrishna, Bashetty K, Srirekha A, Lekha S, Champa. An in vitro evaluation of fracture strength of endodontically treated teeth with simulated flared root canals restored with different post and core systems. J Conserv Dent. 2012 Jul-Sep;15(3):223-7.
9. Juloski J, Apicella D, Ferrari M. The effect of ferrule height on stress distribution within a tooth restored with fibre posts and ceramic crown: a finite element analysis. Dental Materials. 2014 Oct;30(12):1304-15.
10. Kathuria A, Kavitha M, Khetarpal S. Ex vivo fracture resistance of endodontically treated maxillary central incisors restored with fiberreinforced composite posts and experimental dentin posts. J Conserv Dent. 2011 Oct;14(4):401-5.
11. Lertchirakarn V, Palamara JEA, Messer HH. Load and strain during lateral condensation and vertical root fracture. J Endod. 1999 Feb;25(2): 99-103.
12. Martins JNR. Primeiro pré-molar superior com três canais: diagnóstico e tratamento – quatro casos clínicos. Rev Port Estomatol Med Dent Cir Maxilofac. 2011;52:43-51.
13. Mireku AS, Romberg E, Fouad AF, Arola D. Vertical fracture of root filled teeth restored with posts: the effects of patient age and dentine thickness. Int Endod J. 2010 Mar;43(3):218-25.
14. Nassif AC, Tieri F, da Ana PA, Botta SB, Imparato JC. Structuralization of a human teeth bank. Pesqui Odontol Bras. 2003 May;17(1):70-4.
15. Nothdurft FP, Seidel E, Gebhart F, Naumann M, Motter PJ, Pospiech PR. The fracture behavior of premolar teeth with class II cavities restored by both direct composite restorations and endodontic post systems. J Dent. 2008 Jun;36(6):444-9.
16. Pitts DL, Matheny HE, Nicholls JI. An in vitro study of spreader loads required to cause vertical root fracture during lateral condensation. J Endod. 1983;9(12):544-50.
17. Portela CP, Baratto Filho F, Tomazinho FSF, Correr GM, Moro A, Moresca RC. Estudo da anatomia interna dos pré-molares – revisão de literatura. Odonto. 2011 Jan-Jun;19(37):63-72.
18. Seow LL, Toh CG, Wilson Nairn HF. Strain measurements and fracture resistance of endodontically treated premolars restored with all-ceramic restorations. Journal of Dentistry. 2015 Jan;43(1):126-32.
19. Sharath Chandra SM. Sharonlay – a new onlay design for endodontically treated premolar. JCD. 2015 Mar-Apr;18(2):172-5.
20. Souza EM, Pappen FG, Leonardi DP, Flores VO, Berbert FLCV. O papel da anatomia radicular na colocação de pinos pré-fabricados: uma visão endodôntica. Rev Gaúc Odontol. 2007 Jan/ Mar;55(1):77-82.
21. Wilcox LR, Roskelley C, Sutton T. The relationship of root canal enlargement to fingerspreader induced vertical root fracture. J Endod. 1997 Aug;23(8):533-4.
22. Yang SF, Rivera EM, Walton RE. Vertical root fracture in nonendodontically treated teeth. J Endod. 1995 Jun;21(6):337-9.
 Corresponding author:
Corresponding author:
Rosany Laurentina Santos de Carvalho
Rua Dr. Osvaldo Salsa, n. 100, apto 1.501 – Graças
CEP 52011-170 – Recife – PE – Brasil
E-mail: rosanycarvalho@hotmail.com
Received for publication: October 29, 2014
Accepted for publication: September 14, 2014
