










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRSBO (Online)
versão On-line ISSN 1984-5685
RSBO (Online) vol.12 no.3 Joinville Jul./Set. 2015
Case Report Article
Oral rehabilitation of a child with dentinogenesis imperfecta – case report
Kelly Maria Silva MoreiraI; Cibele Aparecida SilvaII; Rayen Milanao DrugowickIII; José Carlos Pettorossi ImparatoIV; Juliana Braga ReisII
I Department of Pediatric Dentistry, School of Dentistry of Piracicaba, State University of Campinas – Piracicaba – São Paulo – Brazil
II Department of Pediatric Dentistry, São Leopoldo Mandic School – Belo Horizonte – Minas Gerais – Brazil
III Department of Pediatric Dentistry, Uniararas/Fundação Hermínio Ometto – Araras – São Paulo – Brazil
IV Department of Pediatric Dentistry, School of Dentistry, University of São Paulo – São Paulo – São Paulo – Brazil
ABSTRACT
Introduction and Objective: To report the clinic case of a 5-yearold boy with presenting yellow-gray teeth and generalized severe tooth crown wear. Case report: After clinical and radiographic examination, he was diagnosed with dentinogenesis imperfecta. After the behavior management, we performed the adequacy of oral environment and diet and oral hygiene instructions. Study models were obtained and then, the rehabilitation treatment was performed through acetate crowns and orthodontic bands. Conclusion: Early diagnosis and treatment are very important in preventing further damage to dental tissues, other oral diseases, and orthodontic changes. Therefore, knowledge of the etiology and family history of the patient is crucial.
Keywords: dentinogenesis imperfecta; child; oral rehabilitation.
Introduction
Odontogenesis is the tooth formation process involving interactions between the epithelium and ectomesenchyme. These interactions are genetically determined and highly regulated, resulting in forming dental and periodontal tissues. The process of dentin formation is called dentinogenesis and occurs by odontoblasts differentiation 11,19.
According to some studies 16,20,21, there might be hereditary changes in dentinal development, affecting the organic matrix and its mineralization. The dentinogenesis imperfecta (DI) is a localized form of mesodermal dysplasia of dentin, which affects both dentitions, occurring most in primary teeth 3,14. With regard to the prevalence, DI signs usually occur in the half number of each offspring with equal frequency between male and female 7.
There are three types of dent inogenesis imperfecta: Type I (dentinal changes associated with osteogenesis imperfecta presence), Type II (only changes in teeth), and Type III (only the teeth are affected, but with varied clinical findings such as pulp exposures and bell-shaped crowns). The presence of enlarged pulp chamber was radiographically observed in patients with type III dentinogenesis, different from types I and II 7,16.
The only similarity of type I and II dentinogenesis imperfecta hinders the diagnosis. Mild forms of the osteogenesis imperfecta may be associated with dentinogenesis imperfecta without diagnosis so that the treatment is postponed 3,8. However, preventive measures must be taken early to avoid fractures and occlusion changes, because teeth with dentinogenesis imperfecta have a reduction in surface hardness 12 and are extremely susceptible to wear 13.
The correct diagnosis enables proper, comprehensive and treatment plan, based on health promotion and in restoring the aesthetic 6,15, self-image 2, and the patient's quality of life 9,17. Early diagnosis and treatment are essential to obtain a favorable prognosis, because late management complicates treatment 18.
This study aimed to describe the dental treatment of a patient with dentinogenesis imperfecta to reestablish the function, vertical dimension, aesthetic, growth, and development of alveolar bone in the vertical direction through orthodontic bands alternatively for rehabilitating the posterior teeth.
Case report
A 5 year-old boy attended the Graduate Clinics of the School of Dentistry of São Leopoldo Mandic (Belo Horizonte, Brazil). His mother agreed with the treatment and signed a free and clarified consent form. This study was submitted and approved by the Institutional Review Board regarding ethical aspects under protocol number #2015/0392.
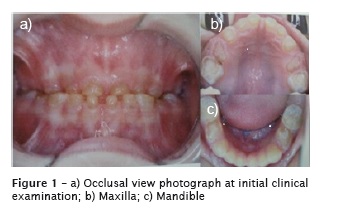
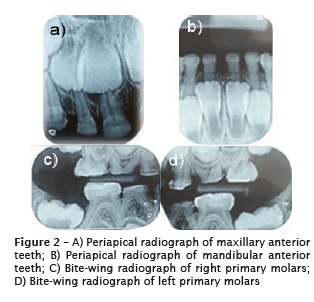
First, at the anamnesis, we gather information on general health. At intraoral clinical examination, the patient showed complete primary dentition At intraoral clinical examination, the patient showed complete primary dentition with yellow-gray teeth and generalized severe wear of tooth crowns (figure 1 A-C). Also, we note the presence of vertical dimension loss. Radiographically, the coronal pulp was retracted and the density of the enamel layer was smaller than normal, because of heavy wear (figure 2 A-D). The patient had very agitated behavior, but no embarrassment because of dental aesthetics. However, the mother reported that he complained about his appearance.
After clinical and radiographic examination, the boy was diagnosed with dentinogenesis imperfecta. At anamnesis, the mother reported that she, her older son, and her father had dentinogenesis imperfecta.
The rehabilitative treatment was the best option because of the large loss of tooth structure and vertical dimension. The topical application of fluoride was performed to decrease dentinal sensitivity, improving toothbrushing.
At the first appointment, the patient underwent behavior management, diet and oral hygiene counseling. Also, plaque disclosing, supervised toothbrushing and prophylaxis was carried out. Moreover, periapical and bitewing radiographs were requested.
At the second appointment, an impression with alginate was taken to obtain study casts.
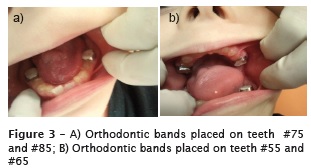
Other prophylaxis and toothbrushing instruction was performed at the third appointment and we opt to reestablish the vertical dimension by placing orthodontic bands (Morelli) on teeth #55, #65, #75 and #85 cemented with glass ionomer cement (Maxxion R, FGM), because of the lack of tooth structure (figure 3 A-B).
After this period, the patience was followedup until mixed dentition. At the first transitional period, the rehabilitation treatment began.
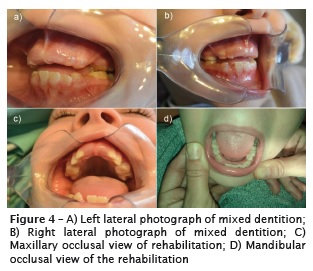
The teeth #52, #53, #55, #62, #63, #65, #73, #74, #75, #83, #84, #85 were rehabilitated with acetate crowns and resin composite (Filtek Z350 XT – 3M ESPE) to reestablish the function and aesthetics of the patient. The teeth #54 and #64 were extracted due to lack of structure for placing post and crown (figure 4 A-D). Space maintainers were installed to prevent space loss.
Discussion
In this case report, imperfect dentinogenesis presented hereditary character, similar to other cases reported by other studies in which this anomaly showed an autosomal dominant inheritance with high penetrance and variable expressivity 3,14,16,20,21.
One of DI clinical features is tooth opacity, ranging from brownish to bluish-gray. Because DI is a mesodermal change, the enamel is normal, but it detaches or breaks due to changes in enamel-dentinal junction. Dentin is severely hypomineralized 5 after exposure, it becomes soft and quickly undergoes wear, reaching the cervical level, which leads to loss of the vertical dimension 6,7, as observed in this case report. The radiographic might show bulb-shaped crowns with obliterated pulp chambers and canals; short and tapered roots; and periapical rarefaction in the primary dentition; but, apparently without pulp exposure or necrosis 1,3,14, similar to which was observed in this case report.
Many approaches can treat DI: direct and indirect restorations with resin composite and placement of stainless steel crowns on posterior teeth 13. Alternatively, we opted to place orthodontic bands on posterior teeth, because of tooth structure loss which made the use of SSCs inviable.
Acetate crowns have been used with composite resin to rehabilitate anterior teeth and prefabricated metal crowns to restore the vertical dimension 7. In this present case report, we use resin composite with acetate crowns because this was a more conservative approach not requiring large preparations. According to some authors, the reestablishment of vertical dimension should be performed immediately 3, as in this present case report.
Similarly to what was observed in other study 17, we noticed heavy wear of the primary teeth, some at gingival level, and we opted by the extraction due to the lack of structure for endodontic therapy and installation of post and crown.
The adhesion of restorative materials is greatly reduced, as reported in other case 4, requiring strict patient's following-up with further oral hygiene and diet instructions, topical application of fluoride and repair of restorations. Thus, both aesthetic and functional rehabilitation positively and psychologically impact on the individual's quality of life 10.
Conclusion
Early diagnosis and treatment of patients with dentinogenesis imperfecta are very important to prevent a more severe destruction of tooth tissues, caries and periodontal disease, and orthodontic changes. Therefore, knowledge of the etiology and familiar history of the patient is crucial.
References
1. Bailleul-Forestier I, Molla M, Verloes A, Berdal A. The genetic basis of inherited anomalies of the teeth. Part 1: clinical and molecular aspects of non-syndromic dental disorders. Eur J Med Genet. 2008 Jul-Aug;51(4):273-91. [ Links ]
2. Biethman R, Capati LR, Eldger N. Dentinogenesis imperfecta: a case report of comprehensive treatment for a teenager. Gen Dent. 2014 Jul- Aug;62(4):18-21.
3. Cardoso T, Cunha R, Cardoso IL. Dentinogênese imperfeita: breve revisão. Rev Port Estomatol Med Dent Cir Maxilofac 2011 Jan-Mar;52(1):52-5.
4. Caseiro CG, Long SM, Chelloti A, Raggio DP, Camargo LB. Dentinogênese imperfeita – relato de caso clínico. Rev Inst Ciênc Saúde. 2009 Jun;27(2):185-8.
5. de La Dure-Molla M, Philippe Fournier B, Berdal A. Isolated dentinogenesis imperfecta and dentin dysplasia: revision of the classification. Eur J Hum Genet. 2015 Apr;23(4):445-51.
6. Devaraju D, Devi BY, Vasudevan V, Manjunath V. Dentinogenesis imperfecta type I: A case report with literature review on nomenclature system. J Oral Maxillofac Pathol. 2014 Sep;18(1):131-4.
7. Freitas KP, Antonio AG, Winx MLP, Castro RAUL, Vianna RBC. Dentinogênese imperfeita tipo III e tipo II em crianças: relato de casos. Rev Odonto. 2008 Jul-Dec;16(32):130-6.
8. Kantaputra PN. Dentinogenesis imperfectaassociated syndromes. Am J Med Genet. 2001 Nov;104(1):75-8.
9. Leal CT, Martins LD, Verli FD, de Souza MA, Ramos-Jorge ML. Case report: clinical, histological and ultrastructural characterization of type II dentinogenesis imperfecta. Eur Arch Paediatr Dent. 2010 Dec;11(6):306-9.
10. Machado CV, Pastor IMO, Telles PDS, Rocha MCBS. Osteogênese imperfeita associada à dentinogênese imperfeita: relato de caso. RFO/UPF. 2012 Sep-Dec;17(3):336-41.
11. Mafra RP, Vasconcelos RG, Vasconcelos MG, Queiroz LMG, Barboza CAG. Desenvolvimento dental: aspectos morfogenéticos e relações com as anomalias dentárias do desenvolvimento. Rev Bras Odontol. 2012 Jul-Dec;69(2):232-7.
12. Min B, Song JS, Lee JH, Choi BJ, Kim KM, Kim SO. Multiple teeth fractures in dentinogenesis imperfecta: a case report. J Clin Pediatr Dent. 2014;38(4):362-5.
13. Rafeek RN, Paryag A, Al-Bayaty H. Management of dentinogenesis imperfecta: a review of two case reports. Gen Dent. 2013 May-Jun;61(3):72-6.
14. Ruschel HC, Modesto A, Marassi CS. Dentinogênese imperfeita: abordagem clínica e relato de casos na dentição decídua. RGO. 2000 Jul-Sep;48(3):147-54.
15. Sapir S, Shapira J. Dentinogenesis imperfecta: an early treatment strategy. Pediatr Dent. 2001 May-Jun;23(3):232-7.
16. Shields ED, Bixler D, El-Kafrawy AM. A proposed classification for heritable human dentin defects with a description of a new entity. Arch Oral Biol. 1973 Apr;18(4)543-53.
17. Silva KOR, Azevedo TDPL. Dentinogênese imperfeita: relato de caso clínico. Rev Odontol Bras Central. 2011;20(55):354-58.
18. Surendra P, Shah R, Roshan NM, Reddy VVS. Dentinogenesis imperfecta: a family which was affected for over three generations. J Clin Diagn Res. 2013 Aug;7(8):1808-11.
19. Thesleff I. Epithelial-mesenchymal signalling regulating tooth morphogenesis. J Cell Sci. 2003 May;116(9):1647-8.
20. Witkop CJ. Hereditary defects of dentin. Dent Clin North Am. 1975 Jan;19(1):25-45.
21. Wi tkop CJ. Amelogenesis imper fect a dentinogenesis imperfecta and dentin dysplasia revisited: problems in classification. J Oral Pathol. 1989 Nov;17:547-53.
 Corresponding author:
Corresponding author:
Kelly Maria Silva Moreira
Rua Alferes José Caetano, 1.858, apto. 41 – Centro
CEP 13400-126 – Piracicaba – São Paulo – Brasil
E-mail: kellynhaodonto@yahoo.com.br
Received for publication: March 12, 2014
Accepted for publication: August 4, 2015
