










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRSBO (Online)
versão On-line ISSN 1984-5685
RSBO (Online) vol.12 no.4 Joinville Out./Dez. 2015
ORIGINAL RESEARCH ARTICLE
Prevalence of caries disease in Pro-Health practices
Ananda da Silva MaganhotoI; Marcelo Eduardo Gracia BauerI; Célia Maria Condeixa de França LopesI; Helena Maria Antunes PaianoI; Denise VizzottoI
I Department of Dentistry, University of Joinville Region – Joinville – SC – Brazil
ABSTRACT
Objective:This research aimed to evaluate the prevalence of caries and cariogenic habits in children living in Jardim Paraíso neighborhood, city of Joinville–SC, where Pro-Health practices have been executed since 2009. Material and methods: Data collection was performed according to the WHO criteria for epidemiological survey. Food and oral hygiene habits of children and socioeconomic characteristics of their caregivers were collected through a questionnaire with closed questions. The sample consisted of 137 children, 69 (50.4%) males and 68 (49.6%) were female. Results: There was statistical significance in relation to intake of cariogenic foods when compared to dmft index, demonstrating positive correlation between the frequency of consumption and caries manifestation. The mean dmft index was 1.61, with a predominance of decayed teeth (92.76%), demonstrating the need for more financial support in public policies for oral health promotion and education in the neighborhood, aiming at the paradigm shifting from curative dental practice to the current approach focused on prevention.
Keywords: caries; children; dmft.
Introduction
The history of caries in human civilization can be described in three different times. The first relates to the pattern of the disease in primitive communities, with low impact on the population, in terms of quantity and severity of the disease, while the second is described by the process industrialization, urbanization, and the introduction of different eating habits, increasing caries prevalence levels 12.
The third 12 refers to the decrease in prevalence and severity of the disease. Despite that the last Brazilian epidemiological survey (SB Brazil 2010) 4 found a 17% reduction in decayed primary teeth and the extensive literature on the subject, dental caries is still a disease raising interest for research. Its distribution occurs differently among regions, but also in relation to the socioeconomic conditions as it involves multiple factors such as oral hygiene habits, diet, and level of education about the disease, among others.
The World Health Organization (WHO) and the International Dental Federation (FDI) stablished the 2000's goal that at least 50% of children between 5 and 6 years of age should be free of caries; 2010's goal was that 90% of the children free from the disease 23.
According to the results of the SB Brazil 2010, the dmft index average is 2.43, for the 5-yr age group in Brazil, and the predominant component was "caries experience", reaching 80% of the index 5.
To the caries prevalence in children requires knowing the etiologic factors of disease, thereby st ructuring specific programs towards the maintenance of children's oral health. Therefore, knowing the factors that affect the caries process allows adopting educational and preventive strategies in oral health since early childhood, reducing the incidence of disease, so that caries-free becomes a normal condition in adulthood 14.
Since 2008, the University of Joinville Region (Univille) elected Jardim Paraíso neighborhood to develop teaching, research and extension activities, to incorporate in the training process of undergraduates from health-care courses the health-disease process approach that addresses social determinants with full health care perspective. The health care courses filled in a proposal for the project "The University at the Service of Health" from Pro-PET Health II and III the Brazilian Ministry of Health and Education approved. The program's actions focused on education and promotion of general and oral health, developed in basic health units, neighborhood, schools, and early-childhood education centers (CEIs)20,22.
The Jardim Paraíso neighborhood has five Basic Units of the Family Strategy (UBSF), but none has a dentist, and the only public reference to oral health available in the neighborhood is the Dental Clinics at the Municipal School Hans Dieter Schmidt 11.
This study aimed to evaluate the prevalence of dental caries in 5 year-old preschool children at the Jardim Paraíso neighborhood (Joinville - SC, Brazil) through dmft index, and relate to the knowledge level of the legal guardians on oral hygiene habits, diet, and socioeconomic status.
Material and methods
This study was approved by the Ethical Committee in Research from Univille under protocol no. #0 486.09 on December 10, 2013.
The survey was conducted with 5 year-old children, of both genders, enrolled in all educational institutions at Jardim Paraíso neighborhood, city of Joinville/SC, Brazil. The neighborhood has two early childhood municipal education centers (CEI Bem-me-Quer and CEI Paraíso da Criança), and three has special agreement with the city: Grupo de Assistência Social Paraíso (GASP), CEI Algodão Doce, and CEI Cantinho da Criança.
The number of 5-year chi ldren in thi s neighborhood was 347, 166 male and 181 female 19. Of these 347 children, 208 were regularly enrolled in pre-school institutions of the neighborhood 19. Exclusion criteria included children aged less or more than 5 years-old at the time of the clinical examination; children whose parents did not sign the informed consent form; children who missed the days of the clinical examination; students not enrolled in the schools and those enrolled in teaching institutions not formalized in the Jardim Paraíso neighborhood.
The research was descriptive, observational, cross-sectional, and analytical conducted at two stages. At the first step, a closed-question questionnaire, containing 24 questions related to hygiene and food habits of the children and the socioeconomic status of families was used.
At the second step, tooth condition was assessed by dmft, available on the site of the Brazilian Ministry of Health 3, adapted according to the needs of this study. The codes and criteria of the survey used the tooth as a measurement unit and the methodology proposed by WHO, according to the Field Team Manual 3.
Data were stored in tables at Microsoft Office Excel 2007 program for descriptive statistics. The following statistical tests were used: Mann-Whitney U test, Chi-square test, and Spearman rank order correlation test.
Results and Discussion
Of the total of 208 children under 5 years of age, 137 (65, 9%) comprised the sample of this study and 71 (34.1%) were excluded. Of these, 51 (24.5%) did not have the Informed Consent signed by the parents (4.80%), ten did not return the questionnaire, and ten (4.80%) missed the clinical examination day. The sample was composed by 50.4% of males and 49.6% of females.
Concerning to tooth condition of 137 children, 78 (56.9%) were caries-free at the time of examination, with dmft index equal to zero, and 43.1% had some tooth decayed, missed, or filled. Of these, 16.8% showed dmft index #1 and #2; 13.2% dmft index #3 and #4; 8.0% dmft index #5 and #6; 8.0% dmft index #5 and #6; 5.1% dmft index #7 to #12 (table I).
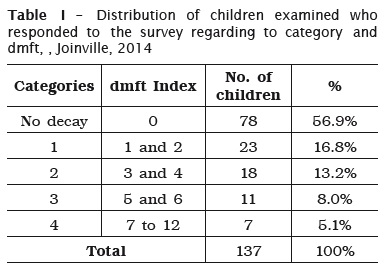
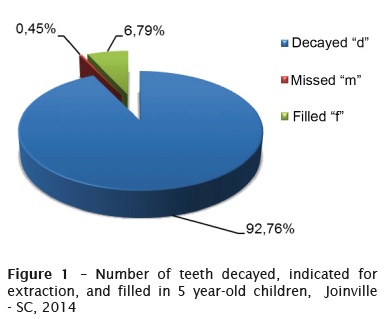
The mean dmft index found was 1.6, with a prevalence of decayed teeth of 92.76% (graph 1). Minimum confidence interval of 1.20; maximum confidence interval of 2.03; sample error of 0.42. This result agrees with the study conducted with 1,374 5-year-old children, in the city of Salvador – BA (Brazil) which found a dmft index of 1.97, with decayed being the largest component (85.78%)1 and also with the data found by the epidemiological survey of oral health SB Brazil 2010, in which the prevalence of decayed teeth was high (80%) 5. However, it is worth noting the significant difference found by the Brazilian survey mean dmft (2.43) with that of this research (1.61) for the same age group. A study conducted with 477 children aged 3 to 5 years had not been restored, showing that the access to dental services is reduced in this age group 2.
In relation to gender and dmft index, Mann- Whitney test showed no statistically significant difference between boys (dmft=1.46) and girls (dmft=1.76%), corroborating the studies found in the literature 13,18. However, this data disagree with the study examining 2,805 children aged from 5 to 6 years and finding differences only at the age of five years, with a higher prevalence of males (55.80%) in relation to dmft 8.
In relation to supervised brushing, most of the children (46.7%) brushed their teeth together with their guardians. Notwithstanding, 38.0% performed oral hygiene alone, and only 5.8% of the guardians brushed their children's teeth, disagreeing with the result of a study on children aged from 2 to 5 years in which the vast majority (76.2%) of the parents were responsible for brushing their children's teeth 10. Children under 6 years-old do not have enough motor skills and understanding to perform oral hygiene alone, needing the aid of an 6,10.
Most (94.9%) used toothpaste on toothbrushing; of these, 70.8% used child toothpaste and 28.5% used adult toothpaste. Concerning to toothbrush, 99.3% of children had his/her own brush; 97.8% were child toothbrushes. Only 13.1% flossed their teeth. These results corroborate data found in the literature. Almost all children (99.2%) had toothbrush; of these, most (81.4%) were child's toothbrush and child toothpaste was the most used for 60.7%, and only 4.2% flossed 10.
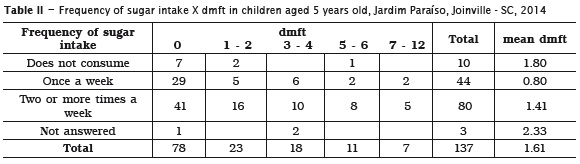
Most of the children (58.4%) consumed sugar food twice or more per week and 7.3% did not consume candy between meals (table II). To compare the frequency of intake of sugary foods with dmft, we used the Spearman test). The z of 3.94 showed conclusive to say that the difference of dmft distributions according to frequency of candy consumption is statistically significant (p <0.005). A sucrose-rich diet offered several times a day between meals will result in a higher early caries experience in children 9,15. Notwithstanding, data found in the literature did not indicate this statistically significant association between high sugar intake with caries appearance 17.
Most of the children (70.8%) consumed sugarsweetened beverages (soft drinks, yogurt, chocolate, artificial juice) two or more times per week, 24.1% once a week, and 3.6% did not consume. The data demonstrate statistical significance when associated with dental caries. The dmft index was higher in those children whose consumption was twice or more times per week. These data are similar to those found by the authors who analyzed the dental caries experience and consumption of sugary foods in 56 preschool children aged 36-78 months. The results revealed that 87.5% of children consumed chocolate milk; of these, 71.4% drank milk with sugar, 92.8% drank soft drinks, and 98.2% natural or artificial juice sweetened with sugar, which led to a statistically positive association between sugar consumption and dmft 21.
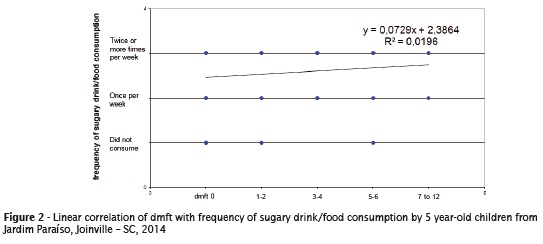
The frequency of intake of sweetened beverages was also compared with the dmft, through the Spearman test. The z was 4.46 and the difference of dmft distributions according to the frequency of consumption of juices and sweetened soft drinks were statistically significant (p <.005), the higher the consumption, the higher is the dmft.
The results of the linear correlation test in relation to the frequency of sweetened food/drink intake showed positive correlation between the high consumption of sugary foods and drink and dmft (figure 2).
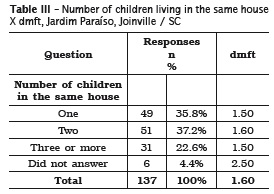
With regard to the number of children living in the same house, 37.2% answered two children, 35.8% only one, and 22.6% three or more children (Table III). We use Spearman test to compare dmft with this data. The z was 8.94 showing statistically significant differences of the dmft distributions according to the number of children living in the same house (p < 0.005), i.e., the presence of two children in the same house predisposes to caries. Only children have lower risk of developing caries compared to the presence of three or more siblings in the same house, that is, the more children living in the same place, the greater id the risk of caries in preschool children 15.
Most families (53.3%) had monthly income around two minimum wages, a significant factor when related to caries disease. Children whose family income less than five minimum wages had 4.18 times higher chance of presenting carious lesions than those with income above five minimum wages 16. With regard to family income, the results agree with socioeconomic standard of the Jardim Paraíso neighborhood, because 36.69% of the population has a monthly income of 1-2 minimum wages, mean of 1.16 minimum wages per month11. The results also corroborates with the fact that housewives and fathers with better professional status tend to have children with lower caries index 7.
Conclusion
According to the methodology applied and the results obtained, it can be concluded that:
• The dmft index of 1.6 in the Jardim Paraíso neighborhood was lower than that found in the Brazilian survey on oral health SB Brazil 2003 and 2010, whose dmft index was 2.8 and 2.3 respectively for the age of 5 years.
• The prevalence of caries in the Jardim Paraíso neighborhood, in the year 2014 was 43.1%, and the component decayed ("c") proved to be prevalent (92.76%), indicating that there is a need for greater access to dental services for the age range studied.
• The behavioral variables such as the frequency of daily toothbrushing, high consumption of sugary foods and drinks as well as the number of children in the house, appear as factors with a statistically significant influence on the dmft in the study.
This study presents information relevant to oral health planning of Jardim Paraíso neighborhood in the city of Joinville / SC, mainly for planning and continuity of the action of Pro-PET Project -. Health, in order to change the local epidemiological status. Also, it is a starting point in relation to the prevalence of caries at 5 years of age in the neighborhood, considering the official methodology proposed by the Ministry of Health and World Health Organization.
References
1. Almeida TF, Cangussu MCT, Chaves SCL, Silva DIC, Santos SC. Condições de saúde bucal de crianças na faixa etária pré-escolar, residentes em áreas de abrangência do Programa Saúde da Família em Salvador, Bahia, Brasil. Rev Bras Saúde Mater Infant. 2009 Jul;9(3):247-52. [ Links ]
2. Boralho SAMFM. Prevalência, gravidade e fatores associados à cárie precoce da infância no distrito de Lisboa. Lisboa. Tese [Doutorado] – Universidade de Lisboa; 2014.
3. Brasil. Ministério da Saúde. Manual da equipe de campo. Brasília, 2009 [cited 2014 Jul 12]. Available from: URL:http://dab.saude.gov.br/ CNSB/sbbrasil/arquivos/SBBrasil2010_Manual_ Equipe_Campo.pdf.
4. Brasil. Ministério da Saúde. SB Brasil 2010: pesquisa nacional de saúde bucal. Brasília, 2011 [cited 2013 Jun 25]. Available from: URL:http:// dab.saude.gov.br/CNSB/sbbrasil/arquivos/Projeto_ SB2010_VersaoFinal.pdf.
5. Brasil. Ministério da Saúde. Secretaria de Atenção à Saúde. Secretaria de Vigilância em Saúde. SB Brasil 2010: pesquisa nacional de saúde bucal: resultados principais. 1. ed. Brasília; 2012. p.116-38.
6. Cascaes AM, Peres KG, Peres MA, Demarco FF, Santos I, Matijasevich A et al. Validade do padrão de higiene bucal de crianças aos cinco anos de idade relatado pelas mães. Rev Saúde Pública. 2011 Aug;45(4):668-75.
7. Castilho ARF, Mialhe FL, Barbosa TS, Puppin- Rontani RM. Influência do ambiente familiar sobre a saúde bucal de crianças: uma revisão sistemática. Jornal de Pediatria. 2013 Mar;89(2):116-23.
8. Cypriano S, Sousa MLR, Rihs LB, Wada RS. Saúde bucal dos pré-escolares, Piracicaba, Brasil, 1999. Rev Saúde Pública. 2003 Apr;37(2): 247-53.
9. Deliberali FD, Brusco EHC, Brusco L, Perussolo B, Patussi EG. Fatores comportamentais envolvidos no desenvolvimento da cárie precoce em crianças atendidas na Clínica de Odontopediatria da Faculdade de Odontologia de Passo Fundo – RS, Brasil. RFO UPF. 2009;14(3):197-202.
10. Ferreira JMS, Bezerra IF, Cruz RES, Vieira ITA, Menezes VA, Granville-Garcia AF. Práticas de pais sobre a higiene bucal e dieta de pré-escolares da rede pública. RGO. 2011;59(2):265-70.
11. Fundação Instituto de Pesquisa e Planejamento para o Desenvolvimento Sustentável de Joinville – IPPUJ. Joinville bairro a bairro. 2013 [cited 2014 Mar 30]. Available from: URL:http:// ippuj.joinville.sc.gov.br/arquivo/lista/codigo/329- Vers%C3%A3o%2B2013.html.
12. Gomes D, Ros MA. A etiologia da cárie no estilo de pensamento da ciência odontológica. Ciênc Saúde Coletiva. 2008 May;13(3):1081-90.
13. Grandella CMF, Oliveira LB, Ardenghi TM, Bönecker M. Epidemiologia da cárie dentária em crianças de 5 a 59 meses de idade no município de Macapá, AP. RGO. 2007 Oct;55(4):329-34.
14. Kriger L. ABOPREV: promoção da saúde bucal. 3. ed. São Paulo: Artes Médicas; 2003.
15. Melo MMDC, Souza WV, Lima MLC, Braga C. Fatores associados à cárie dentária em préescolares do Recife, Pernambuco, Brasil. Cad Saúde Pública. 2011 Mar;27(3):471-85.
16. Peres KGA, Bastos JRM, Latorre MRDO. Severidade de cárie em crianças e relação com aspectos sociais e comportamentais. Rev Saúde Pública. 2000 Aug;34(4):402-8.
17. Ribeiro AG, Oliveira AF, Rosenblatt A. Cárie precoce na infância: prevalência e fatores de risco em pré-escolares, aos 48 meses, na cidade de João Pessoa, Paraíba, Brasil. Cad Saúde Pública. 2005 Nov;21(6):1605-700.
18. Rigo L, Souza EA, Caldas Junior AF. Experiência de cárie dentária na primeira dentição em município com fluoretação das águas. Rev Bras Saúde Mater Infant. 2009 Oct;9(4):435-42.
19. Santa Catarina. Secretaria Municipal de Saúde. População residente por unidade de saúde, faixa etária e sexo – ProGRAB. Joinville; 2013. p.10-12.
20. Schnaider, AK. Projeto da Univille está entre os aprovados pelo Pró-Saúde. NET, Joinville, maio 2008 [cited 2014 Sep 25]. Available from: URL: http://community.univille.edu.br/universouniville/ noticias/prosaude/ 46751.
21. Souza Filho MD, Carvalho GDF, Martins MCC. Consumo de alimentos ricos em açúcar e cárie dentária em pré-escolares. Arq Odontol. 2010;46(3):152-9.
22. Univille. Universidade da Região de Joinville. Projeto A universidade a serviço da saúde. Joinville; 2008.
23. World Health Organization. The World Oral Health Report 2003. Geneva; 2003. [cited 2014 Aug 20]. Available from: URL:http://www.who.int/oral_ health/media/en/orh_report03_ en.pdf?ua=1.
 Corresponding author:
Corresponding author:
Denise Vizzotto
Rua Eduardo Miers, n. 102, apto 504 – Atiradores
CEP 89203083 – Joinville – SC – Brasil
E-mail: dvizzotto@gmail.com
Received for publication: May 5, 2015
Accepted for publication: October 19, 2015
