










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRSBO (Online)
versão On-line ISSN 1984-5685
RSBO (Online) vol.12 no.4 Joinville Out./Dez. 2015
CASE REPORT ARTICLE
Microabrasion and composite resin for re-establishing smile esthetics: a case report
Kamila Oliveira VieiraI; Fernanda Cristina Pimentel GarciaI,II; Gisele Maria Correr NolascoIII; Carla Castiglia GonzagaIII; Priscila Maito RoseiraIII; Fernanda Durski TeixeiraIII; Leonardo Fernandes da CunhaI,III
I Funorte – Brasília – DF – Brazil
II University of Brasília – Brasília – DF – Brazil
III Positivo University – Curitiba – PR – Brazil
ABSTRACT
Introduction:Dental hypomineralization such as dental fluorosis has increased in recent times leading to unaesthetic appearance of teeth. There are different treatment possibilities to improve the aesthetic appearance of hypomineralized enamel described in dental literature. The enamel microabrasion has been a feasible alternative, since it is a fast, safe, conservative, and easy to perform, which promotes good esthetic results. Moreover, this technique is a conservative method that improves the appearance of the teeth by restoring bright and superficial smoothness, without causing significant structural loss. The association of different techniques, such as direct composite resin, can provide good esthetic outcomes, but the etiology, intensity, and depth of stain should be considered to minimize dental structure loss. Objective: To describe an easy technique for managing dental fluorosis using enamel microabrasion in association with direct composite resin. Case report: A mixture of hydrochloric acid and silicon carbide was applied according the manufacturer's instructions. Subsequently, a direct composite resin was applied over the areas where the opacities were more evident. This conservative approach may be considered an interesting alternative treatment to remove fluorosis staining and to improve aesthetic appearance. Conclusion: enamel microabrasion combined with direct composite resin is a conservative and safe alternative method to treat enamel opacities from dental fluorosis. Therefore, this management provides satisfactory aesthetic results for the patient's smile.
Keywords: dental enamel hypoplasia; enamel microabrasion; composite resin; dental esthetics, dental fluorosis.
Introduction
The cause of color change of teeth could be due to extrinsic or intrinsic factors. Extrinsic factors are related to changes caused by factors outside the enamel, such as diet and accumulation of substances in tobacco, wine, coffee and / or foods containing dyes. Intrinsic factors are related to dental developmental defects and systemic conditions, such as enamel hypoplasia, amelogenesis imperfecta, dentinogenesis imperfecta, tetracycline intake during tooth formation, dental trauma during the primary dentition, as well as dental fluorosis, caused by overexposure to fluoride during tooth formation 6.
With the evolution of dental techniques and materials, both the design and procedures changed, and minimal intervention techniques aiming to tooth structure preservation have been now used. Minimally invasive treatments like micro-abrasion and tooth whitening are initial options for treating intrinsic staining of dental enamel. The association between tooth whitening and micro-abrasion can also result in relevant and excellent aesthetic results for patients 15, as well as the association of microabrasion with direct restorations 10.
Microabrasion is a technique that uses an acid (erosive agent) and abrasive agent, which together result in weariness of few microns on the staining and surface irregularities of the enamel without the need to use diamond burs and drills 4. Initially, treatment of dental fluorosis was made by Black, in 1908, using only sandpaper friction to remove the surface enamel stains 1. Microabrasion, associated with an abrasive and erosive agent, began with the use of muriatic acid and heat in the removal of dental fluorosis stains. Since then, many techniques have been described, such as the use of 18% hydrochloric acid associated with fine-grit pumice to form an abrasive paste 5. Subsequently, pastes have been developed containing lower concentrations of Another technique has been described by Mondelli 13, with the use of 37% phosphoric acid replacing hydrochloric acid.
In some situations, the stains are a little deeper and the association with restorative procedures is necessary, so the restorative direct bonding system is also considered a treatment of choice in dental offices for intrinsic enamel stains. The composites allow the tooth structure conservation with excellent cosmetic results 9,10.
The adhesive restorative system has evolved significantly in recent years. In addition, composites have shown excellent optical properties and can reproduce not only the color but also translucity, the texture and gloss of natural teeth, especially nanotechnological resins 7. Recently, the use of nanotechnological materials has been an option for esthetic restorations and can be performed on vital teeth by stained fluorosis associated microabrasion.
Thus, this study aimed to report a case employing the technique of microabrasion associated to direct restoration for removing dental fluorosis stains.
Case report
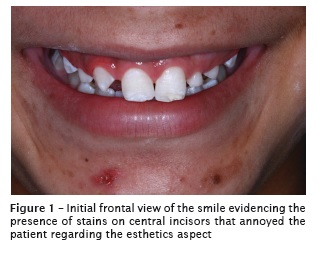
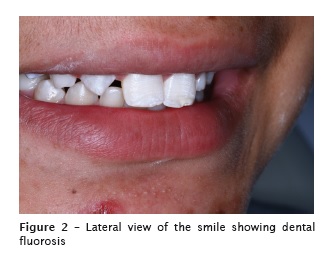
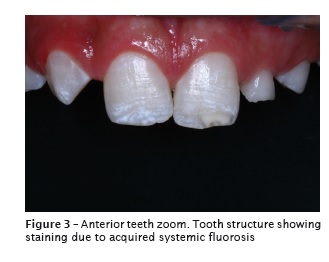
Young patient, male, attended the clinic of the specialization course in Dentistry complaining about dissatisfaction with stains on the teeth (Figures 1 and 2). After anamnesis and clinical examination, the teeth were diagnosed with dental fluorosis (Figure 3).
The proposed treatment was enamel microabrasion. Initially, the dentist must use the personal protective equipment (PPE). Furthermore, it is essential not to forget to protect the patient's eye with glasses, because of the acidic characteristics of the product. Then, the teeth were submitted to tooth prophylaxis. The absolute rubber dam was performed using rubber sheet held in place with an orthodontic elastic ring.
For microabrasion procedure, Whiteness RM (FGM, Joinville, Santa Catarina, Brazil) was used, composed by 6% hydrochloric acid and silicon carbide. The application of acid-abrasive system was performed with rubber cup (TDV – Joinville, Paraná, Brazil), mounted on the low-speed handpiece for initial demineralization of tooth stains. The rubber cup was rubbed on the stained enamel for 10 seconds. Following the manufacturer's instructions, microabrasion procedure may be repeated up to five times in the same appointment. Each tooth was abraded five times at the first appointment. After each application, the tooth surface was washed with water. To verify the need for more product applications, the enamel surface must be kept moist.
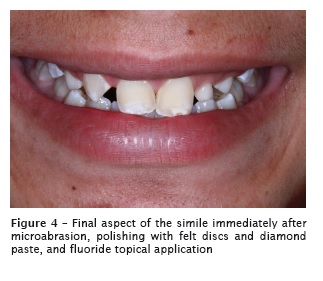
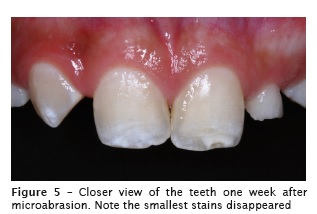
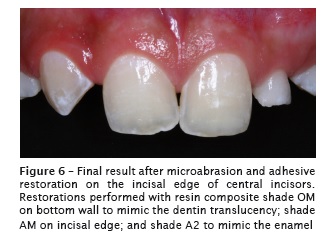
At the second appointment , after one week, the selection of dentin color, enamel and translucent was made (Figures 4 and 5). A second session of microabrasion was executed and a polytetrafluoroethylene-based tape (TDV – Joinville, Paraná, Brasil) was placed on the right central incisor and left lateral incisor to avoid the acid etching of these teeth. The phosphoric acid etching and adhesive application (Gluma Comfort Bond + Desensitizer – Heraeus Kulzer, Hanau, Germany) was applied then light-cured (Poly Wireless – Kavo Kerr Group, São Paulo, Brazil) according to manufacturer's recommendations. Then, dentin resin shade OM (Charisma Diamond – Heraeus Kulzer), was applied, leaving a space in the incisal region to characterize this area of the tooth. A more translucent resin was placed on this area (shade AM – Charisma Diamond), characterizing its hue and translucency of the incisal edge. A single layer of resin shade A2 (Charisma Diamond – Heraeus Kulzer) ) was applied on the labial surface with the aid of a brush (Kota – size #4A) prior to final light-curing. The result immediately after completion of the restoration can be seen in Figure 6.
At the next appointment, the finishing and final polishing was procedure. The sequence of Sof- Lex discs with sequential particle size (3M ESPE, Seefeld, Germany) was applied, and then, rubber cups (ZZag) and felt rods with resin composite polishing paste (Diamond Excel - FGM) ) were used to promote the final gloss.
The final aspect of the restoration on the hypoplastic stain can be seen in Figures 7, 8 and 9.



Discussion
To achieve good results in cases of dental enamel microabrasion, various aspects must be considered. Proper diagnosis and treatment plan should be considered initially. In cases such this reported here, the history and age of the patient are fundamental to the decision between a more conservative or more invasive treatment. According to Furuse et al. 10, a more conservative approach should be preferred at first, wherever possible. Thus, the enamel microabrasion treatment was elected to start the treatment in this case report 10.
Dental microabrasion is a technique proven by several authors to be safe, simple, effective, of low cost, and with exceptional results in cases of superficial enamel stains. The microscopic layer of enamel surface is removed and the discoloration disappears irreversibly 14,15. The literature shows that, on average, for each application the erosive and abrasive removed about 25 microns 8,17, thus restricted to the enamel.
Different techniques can be used depending on the erosion/abrasive agent used. In the case reported herein, the material based on hydrochloric acid and silicon carbide is preferred because of it is commercially available, rather than a phosphoric acid/pumice paste that should be prepared. However, Meireles et al. 12 compared the hydrochloric acid/ silicon carbide technique with the phosphoric acid/ pumice technique and found that both techniques are effective and safe. Thus, the chosen technique will depend on the preference of the practitioner.
In some cases after microabrasion, a more yellowish appearance of the tooth can be observed. This occurs due to the enamel weariness, of micrometers, making dentin more evident 76. In such cases, the tooth whitening can be indicated 2. In the case presented here, the patient was too young, so that whitening was contraindicated. Also, tooth color was not a complaining neither form him nor for his Family.
Due to the greater extent of the stain on the incisal edge of the left central incisor, direct restorative treatment was elected. Many studies demonstrate satisfactory cosmetic results of composites in anterior teeth in different situations, either in fractures, diastema closure, or hypocalcifications, or hypoplasia. The direct adhesive restorative systems provide the following advantages: minimal wear of tooth structure, good clinical durability, fast to perform. Furthermore, direct resin composites have lower cost and are reversible 9,10.
The restorative material used in this case presents nanoparticles. Materials with such particles provide smoother surface and thus favor the results after polishing and brushing. The resins containing nanoparticles tend to show less brightness loss and smaller increase of surface roughness over time 3. Thus, the longevity of such restorations tend to be favored by the properties of these materials.
The long-term monitoring of the patient is fundamental to the success of treatment 11. Therefore, the referral to orthodontic treatment and periodic controls were scheduled.
Enamel microabrasion associated with direct resin composite restorations can be considered a conservative and safe treatment to remove fluorosis stains, improving tooth esthetics.
References
1. Black GV. A work on operative dentistry. The pathology of the hard tissues of the teeth. Chicago: Medico-Dental Publishing Company; 1908. [ Links ]
2. Briso A, Lima A, Goncalves R, Gallinari M, Santos PD. Transenamel and transdentinal penetration of hydrogen peroxide applied to cracked or microabrasioned enamel. Oper Dent. 2013.
3. Costa J, Adams-Belusko A, Riley K, Ferracane JL. The effect of various dentifrices on surface roughness and gloss of resin composites. J Dent. 2010;38(2):123-8.
4. Croll TP, Cavanaugh RR. Enamel color modification by controlled hydrochloric acidpumice abrasion. I. Technique and examples. Quintessence Int. 1986;17(2):81-7.
5. Croll TP, Cavanaugh RR. Enamel color modification by controlled hydrochloric acid-pumice abrasion. II. Further examples. Quintessence Int. 1986;17(3):157-64.
6. Cunha LF, Tomita NE. Dental fluorosis in Brazil: a systematic review from 1993 to 2004. Cad Saúde Pública. 2006;22(9):1809-16.
7. Cunha LF, Valeretto TM, Pirolo R, Mondelli J, Furuse AY, Gonzaga CC et al. Free-hand stratification with composite resins for the closure of anterior diastema. RSBO. 2012;9:334-9.
8. Dalzell DP, Howes RI, Hubler PM. Microabrasion: effect of time, number of applications, and pressure on enamel loss. Pediatr Dent. 1995;17(3): 207-11.
9. Furuse AY, Cunha LF, Runnacles P, Pirolo R, Zielak JC. Using chemical vapor deposition diamond finishing burs for conservative esthetic procedures. General Dentistry. 2013;61:75-7.
10. Furuse AY, Cunha LF, Valeretto TM, Mondelli RFL, Mondelli J. Tratamentos conservadores por meio de microabrasão do esmalte. Revista Dental Press de Estética. 2007;4:54-63.
11. Furuse AY, Herkrath FJ, Benetti AR, Mondelli J. Multidisciplinary management of anterior diastemata: clinical procedures. Pract Proced Aesthet Dent. 2007;19(3):185-91.
12. Meireles SS, Andre DA, Leida FL, Bocangel JS, Demarco FF. Surface roughness and enamel loss with two microabrasion techniques. J Contemp Dent Pract. 2009;10(1):58-65.
13. Mondelli J, Bastos MTAA, Franco EB. Microabrasão com ácido fosfórico. Rev Bras Odontol. 1995;52(3):20-2.
14. Sundfeld RH, Croll TP, Briso AL, de Alexandre RS, Sundfeld D. Considerations about enamel microabrasion after 18 years. Am J Dent. 2007;20(2):67-72.
15. Sundfeld RH, Franco L, Gonçalves R, de Alexandre R, Machado L, Neto D. Accomplishing esthetics using enamel microabrasion and bleaching: a case report. Oper Dent. 2013;Inpress.
16. Sundfeld RH, Rahal V, de Alexandre RS, Briso AL, Sundfeld Neto D. Smile restoration through use of enamel microabrasion associated with tooth bleaching. Compend Contin Educ Dent. 2011;32(3):53-7.
17. Waggoner WF, Johnston WM, Schumann S, Schikowski E. Microabrasion of human enamel in vitro using hydrochloric acid and pumice. Pediatr Dent. 1989;11(4):319-23.
 Corresponding author:
Corresponding author:
Leonardo Fernandes da Cunha
Universidade Positivo
Rua Professor Pedro Viriato Parigot de Souza, 5.300 – Campo Comprido
CEP 81280-330 – Curitiba – PR – Brasil
E-mail: cunha_leo@me.com
Received for publication: August 12, 2015
Accepted for publication: September 29, 2015
