










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRSBO (Online)
versão On-line ISSN 1984-5685
RSBO (Online) vol.12 no.4 Joinville Out./Dez. 2015
CASE REPORT ARTICLE
Endodontic retreatment of dens invaginatus: clinical and radiographic report
Bruno CrozetaI; Allan AbuabaraII; Bruno Marques-da-SilvaI; Jessica VavassoriI; Flares Baratto-FilhoI,III; Denise P. LeonardiI
I Department of Dentistry, Positivo University – Curitiba – PR – Brazil
II Joinville Municipal Authority, Health Division – Joinville – SC – Brazil
III Department of Dentistry, University of Joinville – Joinville – SC – Brazil
ABSTRACT
Introduction and Objective: Dens invaginatus, a developmental malformation resulting from the invagination of enamel, has been associated with increased prevalence of pulpal and periapical diseases. Case report:This anomaly is classified according to the severity (types I-III). Management of type III dens invaginatus is complex and an endodontic challenge. This case report describes the management of the endodontic retreatment type III dens invaginatus in a maxillary lateral incisor. Conclusion: Nonsurgical treatment can be effective to treat type III dens invaginatus. CBCT is an important diagnostic tool that allowed the management of such case.
Keywords: tooth abnormalities; dental pulp cavity; dens in dente; incisor; root canal therapy.
Introduction
Dens invaginatus, or dens in dente, is a developmental malformation resulting from the invagination of enamel organ into the dental papilla. Oehlers 4, in 1957, classified these defects according to their severity. In type I, the enamel invagination is confined in the crown as a blind sac; in type II, the enamel-lined invagination invades the root but remains confined within it as a blind sac, and it may communicate with the dental pulp. There are two variations of type III: the invagination extends from the crown to the apex forming a second foramen in the apical area, or the invagination forms a second foramen somewhere in the periodontal ligament. The enamel may line the type III invaginations completely, and, in some circumstances, the cementum may cover the invagination apically 4.
Dens invaginatus has been associated with increased prevalence of pulpal and periapical diseases 8. Management of dens invaginatus is complex and an endodontic challenge 8,9. The objective of this case report was to describe the complex management of the endodontic retreatment of type III dens invaginatus in a maxillary lateral incisor.
Case report
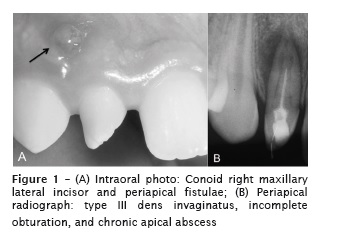
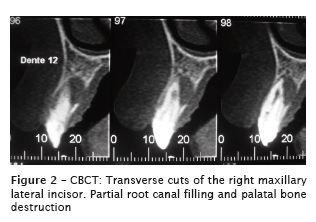
A 12 year-old boy was referred to the School of Dentistry of Positivo University for endodontic retreatment of the right maxillary lateral incisor. The patient's parents were verbally informed and signed the consent form agreeing with the case documentation. Contributory diseases were not reported. Clinically, the crown of the right maxillary lateral incisor presented conical aspect. A gingival fistula was observed (Figure 1A). A vitality test of the tooth was negative. The periapical radiograph revealed incomplete root filling, type III dens invaginatus and chronic apical abscess (Figure 1B). Due to obturation failure, cone-beam computed tomography (CBCT) was requested to evaluate the root canal morphology, locating and identifying root canals (Figure 2). Axial, coronal, and sagittal images were retrieved from CBCT analysis (i-CAT, Imaging Sciences International, Hatfield, PA, USA). The CBCT unit in this study used a 14-bit grayscale and had a voxel size of 0.2mm. The CBCT revealed three root canals, distal-palatal (DP), mesial-buccal (MB), and a middle canal in a flattened area.
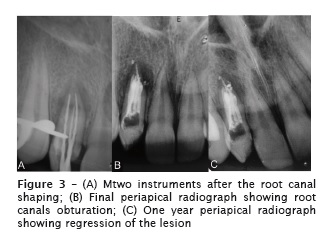
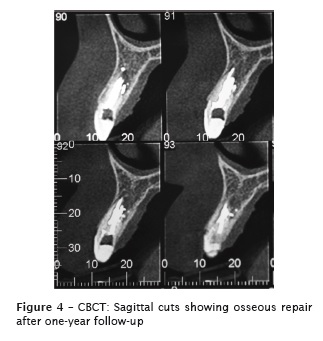
After local anesthesia, nonsurgical root canal treatment was initiated and completed in two sessions. Endodontic access to the cavity was prepared on the palatal surface. The retreatment was made with Mtwo retreatment file #25 (VDW, Munchen, Germany) and the canal yielded purulent fluid exudates. The root canal was prepared by using crown-down technique with Mtwo instruments (VDW, Munchen, Germany) up to size #35.04 (middle canal), #50.04 (distal-buccal), and #60.02 (mesialbuccal) (Figure 3A). The irrigant, 2.5% Sodiumhypochlorite solution, was delivered carefully and passively. A final irrigation with 17% EDTA was performed for 5 minutes. After chemo-mechanical preparation and drying of the root canal system, a calcium hydroxide paste (Calen, SSwhite, Rio de Janeiro, Brazil) was introduced with a lentullo drill to prevent antibacterial activity (Dentsply-Maillefer, Maillefer, Switzerland). After 3 weeks, the patient returned without pain. Regression of the fistulae was observed. Thermomechanical root canal obturation was performed (Gutta Condensers, Dentsply Maillefer) with AH Plus cement (Dentsply-Maillefer) (Figure 3B). One year after the treatment, an X-ray (Figure 3C) was made and regression of the lesion was found. CBCT detected the regression of the lesion and the proper osseous repair (Figure 4).
Discussion
Dental anomalies, including dens invaginatus, can be present in a significant number of people 1. In a recent study, the tooth prevalence of this dental anomaly was found to be 0.4% 7. This anomaly can be present in 2.40-2.95% of people 1,2. Teeth most affected are maxillary lateral incisors and bilateral occurrence is not uncommon3. CBCT may aid the diagnosis as well as the management plan and follow-up of teeth with this developmental anomaly 10.
The treatment of the dens invaginatus varies depending on the invagination types. According Ozbas et al. 6, type I cases can be treated with preventive sealing, filling of the invagination, or root canal therapy. Type II cases can be treated with root canal therapy, which may involve the removal of the anomalous tissue from the pulp space. For treatment-resistant type II cases, the tooth can be treated in association with periapical surgery and retrofilling. Type III cases in which the invagination ends at the apical foramen can be treated likely to type II cases. For type III cases in which the invagination opens somewhere in the periodontal ligament, both the necrotic pulp canal and the invagination can be obturated and, in some cases, periapical surgery can be done. In certain cases, the vitality of pulp tissue can be maintained while the invagination is obturated, and sometimes surgery can be performed in the apex of invagination. Intentional replantation can be attempted as a last approach when conventional and surgical treatments are ineffective in solving the periapical inflammation 6.
Ortiz et al. 5 present a case report of a maxillary lateral incisor having dens invaginatus in which both nonsurgical and surgical treatment was performed. In this case, after the diagnosis of type III dens invaginatus, firstly it was opted for nonsurgical endodontic retreatment. After root canal therapy, clinical and radiographic signs and symptoms regressed, thus surgical procedure was discarded.
The present report indicates that nonsurgical treatment of type III dens invaginatus cases can be successful. CBCT is a diagnostic tool that may allow for the management of such teeth with complex anatomy.
References
1. Gupta SK, Saxena P, Jain S, Jain D. Prevalence and distribution of selected developmental dental anomalies in an Indian population. J Oral Sci. 2011;53(2):231-8. [ Links ]
2. Hamasha AA, Alomari QD. Prevalance of dens invaginatus in Jordanian adults. Int Endod J. 2004;37(5);307-10.
3. Hülsmann M. Dens invaginatus: aetiology, classification, prevalence, diagnosis, and treatment considerations. Int Endod J. 1997;30(2):79-90.
4. Oehlers FA. Dens invaginatus (dilated composite odontome). I. Variations of the invagination process and associated anterior crown forms. Oral Surg Oral Med Oral Pathol. 1957;10(11):1204-18.
5. Ortiz P, Weisleder R, Villareal de Justus Y. Combined therapy in the treatment of dens invaginatus: case report . J Endod. 2004; 30(9):672-4.
6. Ozbas H, Subay RK, Ordulu M. Surgical retreatment of an invaginated maxillary central incisor following overfilled endodontic treatment: a case report. Eur J Dent. 2010;4(3):324-8.
7. Patil S, Doni B, Kaswan S, Rahman F. Prevalence of dental anomalies in Indian population. J Clin Exp Dent. 2013;5(4):e183-6.
8. Robazza CR, Motta JC, de Carli ML, de Oliveira Pedreira FR, Hanemann J. Endodontic retreatment of dens invaginatus presenting with gutta-percha overfilling at the attached gingiva and chronic apical periodontitis: unusual clinical report. J Contemp Dent Pract. 2013;14(3):556-9.
9. Subbiya A, Geethapriya N, Pradeepkumar AR, Vivekanandhan P. An unusual type II dens invaginatus with calcified canals in a maxillary lateral incisor – a case report. J Clin Diagn Res. 2013;7(9):2084-5.
10. Vier-Pelisser FV, Pelisser A, Recuero LC, Só MV, Borba MG, Figueiredo JA. Use of cone beam computed tomography in the diagnosis, planning and follow up of a type III dens invaginatus case. Int Endod J. 2012;45(2):198-208.
 Corresponding author:
Corresponding author:
Bruno Crozeta
Rua Professor Pedro Viriato Parigot de Souza, n. 5.300 – Campo Comprido
CEP 81200-100 – Curitiba – PR – Brasil
E-mail: brunoendodontia@gmail.com
Received for publication: August 28, 2015
Accepted for publication: September 29, 2015
