










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRSBO (Online)
versão On-line ISSN 1984-5685
RSBO (Online) vol.13 no.2 Joinville Abr./Jun. 2016
CASE REPORT ARTICLE
Correction of gummy smile prior to restorative procedures: case report
Felipe Rychuv SantosI; Fernanda Torres ZamboniI; Paula Sayuri YamaguchiI; Carmen Lucia Muller StorrerI; Fernando Henrique Ruppel OsternackI; Naylin Danyele de OliveiraI; Tatiana Miranda DeliberadorI
I Department of Dentistry, Positivo University – Curitiba – PR – Brazil
ABSTRACT
Introduction and Objective: Techniques for aesthetic purposes are being frequently used in dental practice due to social context. These techniques can be used to correct concomitant disharmonies in smile. This clinical case aimed to provide a harmonious smile combining the techniques of gingivoplasty and direct veneers on the maxillary anterior teeth. Case report: The gingivoplasty with clinical crown augmentation sought to correct defects present in toothgingival anatomy, resulting in a realignment of the gingival contour. Conclusion: The direct veneer technique with composite resins was elected for closing the interincisal diastema and correction the size of the involved teeth, providing a more aesthetic dental anatomy.
Keywords: gingivoplasty; esthetics dental; dental veneers.
Introduction
The appearance is relatively important in the individuals' acceptance in to society. The face is the body's part that most appear, evidencing the importance of esthetic dental procedures for correcting the smile 13.
The smile involves muscle and lip movements and exposure of teeth, gingiva, and periodontal structure. Based on these information, the dentist can correct the imperfections of this system, searching for a more harmonic smile.
The periodontal and gingival structures exposed during the smile can be classified according to the height of the exposed gingival tissue: high smile – more than 4 mm of exposure; medium smile – from 3 to 4 mm of exposure; low smile – 3 mm of exposure 10.
This exposure can be related to the vertical excess of the maxilla, interlabial space increased during rest, problems in the alveolar bone formation, tooth eruption without exposing the total curvature of the crown at cervical region, hereditary causes, dense or malpositioned lip frenulum, marked facial muscle tonus, gingival hyperplasia and inflammation 7.
The gingivoplasty aims to correct esthetically the gingival excess, reestablishing the biological and physiological space 13. Medium and high gingival exposure are also called 'gummy smile", which can be corrected by gingivoplasty. To perform gingivoplasty correctly, the dentist should consider: the techniques, gender, age, and race of the individual. Females shows during the smile, the exposure of the tooth-gingival limit more frequently than males. Young people have greater and stronger muscle tonus, and consequently, tend to show more tooth structures during smile than the elderly. Because of the lip shape and volume of black people, they exhibit less maxillary gingiva during smile than white people 6.
Among other indications for gingivoplasty are: the correction of the gingival architecture, clinical crown augmentation, hyperplasia correction, and elimination of the melanin pigmentation. However, gingivoplasty is contraindicated for patients with systemic problems, lack of bacterial control with or without inflammatory process, lack of remaining keratinized gingiva. Among gingivoplasty advantages are: esthetic recovery, decreasing of probing, to favor tooth brushing, and simple surgical technique.
The disadvantages of this procedure are extensive surgical site and healing by second intention 12,15.
The introduction of the resin composites as esthetic restorative material for anterior teeth is one of the most significant advancements in cosmetic dentistry. The evolution of the adhesive systems and the mechanical properties of the resin composites provide a more conservative treatment. The composites, previously sold in a single shade, were improved and thus now enable to mimic the optical characteristics of the tooth structures 14.
The direct adhesive restorations in anterior teeth may be indicated to alter the shape and width/length ratio of one tooth or more teeth to close spaces, as diastemas 1. The diastemas are defined as spaces or lack of contact among maxillary or mandibular teeth, most prevalent in anterior teeth 16.
The indication of direct veneers should follow many aspects: the quality and amount of remaining tooth structure, degree of discoloration, extension of the compromised area toward the periodontal complex, positioning and aligning of teeth, and patient hygiene 14. This restorative procedure is contraindicated in cases of high tooth darkening (because of difficulty in masking the background color), parafunction, deficiency during occlusion (risk of restoration fracture), deleterious oral habits, periodontal problems, and poor tooth positioning (tooth crowding and giroversion) 2,14.
The advantages of this procedure include the easy, safe, and effective repair, no laboratorial phase, decreasing the costs when compared with indirect veneers, no necessity of provisional crowns, and impressions. The chair time depending on the operator's ability, which may be shorter than that of indirect veneers. Generally, direct veneers are reversible because the preparation is more conservative than that of indirect veneers and sometimes no preparation is required. These disadvantages include the increased chair time depending on the professional's ability, smaller resistance to wear, blister formation, which may lead to staining and degradation. Microparticulate composites are susceptible to cleavage 2.
We emphasize the importance of good instruction of the patient about the expected results, mainly in large restorations because this treatment many times will modify the individuals' appearance, demanding caution in consider the patients' opinion rather than that of the professional 11.
This clinical case report aims to provide a harmonic smile associated with gingivoplasty and direct veneer of the maxillary anterior teeth.
Clinical case report
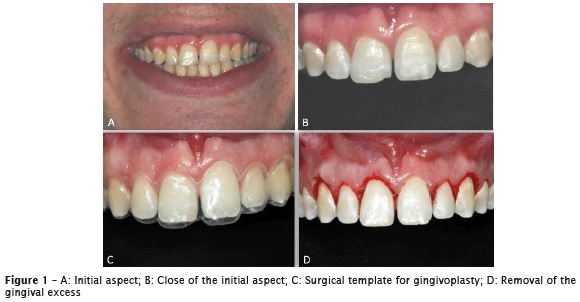
A male individual, V.L., aged 23 years sought treatment at the Integrated Clinics of Positivo University. At clinical examination, the gummy smile was detected (4 mm of exposure), with initial probing of 1.5 mm, without bleeding, interincisor diastema, short sound crowns, fracture of the incisal-mesial edge of tooth #11, which was corrected during the first appointment, and vestibularization of tooth #21. The initial smile aspect exhibited marked maxillary gummy smile, with irregular gingival architecture of the central incisors and inter-incisor diastema (figures 1A and 1B). The amount of attached gingiva was evaluated. The patient was submitted to alginate impression to obtain the study cast to construct a surgical template for the gingival surgery (figure 1C).
The local anesthesia comprised mepivacaine 2% with epinephrine 1:1000.000, by infiltrative technique complemented by the local anesthesia of the distal papillae from the right to left maxillary premolar. Then, reference points were marked with the aid of a periodontal probe on the teeth #11, #12, #13, #22, and #23, taking into consideration the tooth morphology, the gingival zenith, and the amount of gingiva to be removed. The intra-sulcus incision followed this aforementioned reference points to remove the excess gingiva completely (figure 1D).
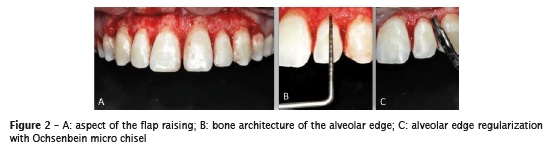
The total flap was raised with the aid of Molt dissector to expose the concave tooth arch, enabling to see the labial bone tissue (figure 2A). The periodontal probing enabled to visualize the distance of the biological space (figure 2B), which should be kept in 3 mm. The alveolar bone was shaped with the aid of Ochsenbein micro chisels and determined the correct enamel-cementum-bone distance (figure 2C).
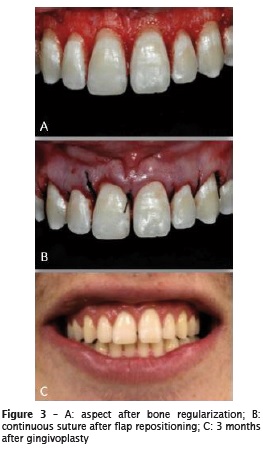
After the gingivoplasty and alveolar bone regularization (figure 3A) the flap was repositioned and sutured continuously (figure 3B). After three months of healing (figure 3C), the restorative procedure was started through light-cured resin composite. To plan the diastema closure, an impression was made to obtain a study cast which was waxed-up for studying the case predictability (figure 4A).
Prior to the restorative procedure, the patient undergone two appointments for tooth whitening with 35% hydrogen peroxide (Whiteness HP Maxx, FGM). Color selection was executed by light-curing small increments of resin composite on the labial surface of the central incisor without previous adhesive system (figure 4B). The shades of resin composite chosen were A1, A2 EN, and TG (Amelogen Plus - Ultradent) (figure 4C).

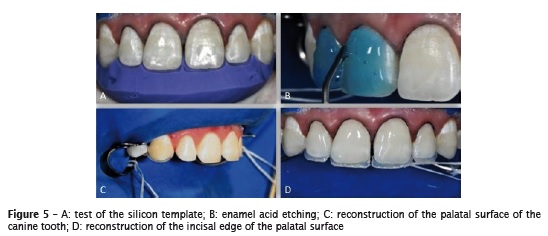
After the modified absolute isolation with the clamps positioned on the second premolars, a retractor thread sized #00 was placed (figure 5A). Next, the labial, palatal and proximal surfaces from right to left canine teeth were etched with 37% phosphoric acid for 1 minute (figure 5B) followed by the application of the adhesive system Foto Adper Scothbond (3M ESPE).
A silicon template was constructed to aid in the restorative procedure. The palatal surface was made with shade EM, to obtain the support for the stratification of the subsequent resins (figure 5C and 5D).
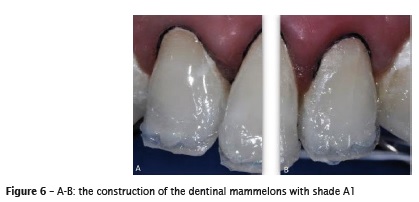
Both the dentin and the dentinal mammelons were made with shade A1 (figure 6). The shade A2 was used in the canine teeth because they are darker. Then, the translucent shades EN and TG were applied to end the enamel layer.
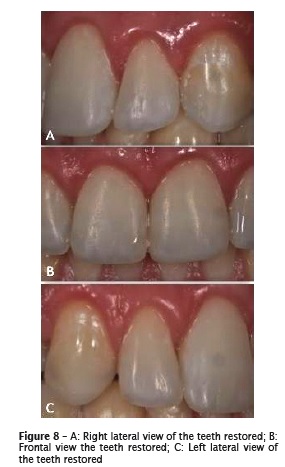
The finishing and polishing procedures were executed one day after the reconstruction with diamond points, sandpaper discs, abrasive points, and felt discs (figures 7, 8, and 9).


Discussion
The association of periodontal surgery with restorative procedures demonstrate satisfactory results for the functional and esthetic rehabilitation of the smile, increasing the patient's self-stem and well-being 15.
The use of direct resin composite for esthetic procedures is a fast, low cost, and effective alternative for many situations such as conoid teeth or teeth showing height/width imbalance. The use of the silicon template constructed with the aid of the diagnosis wax-up enable determining the height/width ratio following the esthetic standards, resulting in fast work with predictability 8.
Currently, many surgical procedures are available for the proper management of the periodontal tissue aiming at stablishing the tooth-gingival esthetic standards together with restorative procedures. The most used periodontal procedures are clinical crown augmentation of the maxillary anterior teeth performed only on the gingival tissue, or associated or not with the bone tissue. The esthetic appearance changes and commonly the patients are surprised with the new size of the teeth. To avoid problems or disappointments after treatment, mock-up and wax-up are powerful tools for demonstrating the possible outcomes for the patient. Also, the air passage during speech is also modified when the diastema is closed; thus, the phonetic assessment is advised. The adaptation to the new condition normally occurs in few days. Periodical following-up appointments favor better esthetic and functional outcomes at long term 5.
Cardoso et al. (2011) used direct veneers and tooth whitening and affirm that to follow classic guidelines of rehabilitative protocols, to know and manage the physical properties of the restorative materials, and to respect the ethical guidelines of minimally invasive dentistry promotes a highly satisfactory outcome, returning the harmony to the smile and plain satisfaction to the patient 3.
Kubo (2011), in retrospective longitudinal clinical trials on resin composite restoration concluded that at least 60% of the restorations would survive more than 10 years when the materials were applied correctly and policies of proper maintenance were employed, capable of increasing the resin composite restoration longevity and increasing the patient's general health 9.
Even if direct resin composite veneers cannot be considered as definitive restorations, in most cases and depend on the operator's ability, they provide pleasant and compensating outcomes 2.
Conclusion
The association of esthetic dental procedures, involving more than one specialty, such as operative dentistry and periodontics, can be favorable in cases of tooth-gingival correction is required.
The use of templates, both to guide the gingivoplasty and the resin composite restoration provided a fast work with predictability.
The direct restorative technique with the use of resin composites, when correctly indicated, is a very satisfactory treatment alternative with main advantages of tooth structure preservation and easy technique 4.
References
1. Baratieri LN, Araujo Junior EM, Monteiro Junior S, Vieira LCC. Caderno de dentística: restaurações adesivas diretas, com resinas compostas, em dentes anteriores. 1. ed. São Paulo: Livraria Santos Editora; 2002. p. 2-6. [ Links ]
2. Baratieri LN, Monteiro Junior S, Andrada MAC, Vieira LCC, Cardoso AC, Ritter AV. Estética – restaurações adesivas diretas em dentes anteriores fraturados. São Paulo: Livraria Santos Editora; 1998.
3. Cardoso PC, Decurcio RA, Pacheco AFR, Lúcio JE, Monteiro LJE, Ferreira MG et al. Facetas diretas de resina composta e clareamento dental: estratégias para dentes escurecidos. Rev Odontol Bras Central. 2011;20(55):341-7.
4. Chimeli TBC, Pedreira APRV, Souza TCP, Maciel M, Paula LM, Garcia FCP. Tratamento restaurador de diastemas anteriores com restaurações diretas em resina composta: relato de caso. Revista Dentística online. 2011 Jan/Mar;(20):54-7.
5. Cunha LF, Mondelli J, Furuse AY. Planejamento e considerações pré e pós operatórias no fechamento de diastemas. Rev Bras Odontol. 2011 Jan/ Jun;68(1):12-15.
6. Duarte CA. Conceito de estética. In: Duarte CA, Castro MVM. Cirurgia estética periodontal. 1. ed. São Paulo: Livraria Santos Editora; 2004. p. 1-2.
7. Dutra MB, Ritter DE, Borgatto A, Derech CA, Rocha R. Influência da exposição gengival na estética do sorriso. Dental Press J Orthod. 2011;16(5):111-8.
8. Holanda DBV, Simões DMS, Khalili JB. Recontorno cosmético em dentes anteriores superiores: relato de caso clínico. Rev Dental Press Estét. 2006 Jan/Feb/Mar;3(1):49-58.
9. Kubo S. Longevity of resin composite restorations. Japanese Dental Science Review. 2011;47:43-55.
10. Mikami I. An evaluation of the functional lip posture. Shigaku. 1990;78:339-76.
11. Mondelli J. Estética e cosmética em clínica integrada restauradora. São Paulo: Quintessence Editora; 2003. p. 3.
12. Ottoni J, Magalhães LF. Cirurgias periodontais básicas. In: Ottoni J, Magalhães LF. Cirurgia plástica periodontal e periimplantar. 1. ed. São Paulo: Editora Artes Médicas; 2006. p. 119-120.
13. Pedron IG, Estevam R, Utumi ER, Leopoldo PN, Silva LPN, Moretto LEML et al. Cirurgia gengival ressectiva no tratamento da desarmonia do sorriso. Rev Odontol Bras Central. 2010;18(48):87-91.
14. Souza Junior MHSE, Carvalho RM, Mondelli RFL. Odontologia estética, fundamentos e aplicações clínicas – restauração com resina composta – I/00. 1. ed. São Paulo: Livraria Santos Editora; 2000.
15. Sousa SJB, Magalhães D, Silva GR, Soares CJ, Soares PFB, Santos Filho PCF. Cirurgia plástica periodontal para correção de sorriso gengival associada a restaurações em resina composta: relato de caso clínico. Rev Odontol Bras Central. 2010;19(51):362-6.
16. Tanaka O. Má oclusão. Simplesmente má oclusão. J Bras Ortodon Ortop Facial. Jul/Aug 2000;V(28)6-10.
 Corresponding author:
Corresponding author:
Felipe Rychuv Santos
Rua Prof. Pedro Viriato Parigot de Sousa, 5.300
Campo Comprido
CEP 81280-330
Curitiba – PR
E-mail: ferychuv@gmail.com
Received for publication: November 19, 2016
Accepted for publication: February 24, 2016
