










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRSBO (Online)
versão On-line ISSN 1984-5685
RSBO (Online) vol.13 no.2 Joinville Abr./Jun. 2016
CASE REPORT ARTICLE
Digital planning for smile reconstruction with ceramic laminates: case report
Giulian Lennon de MacêdoI; Cristóvão José de Lima Silva FilhoI; Iris DurãesI; Carmen de Andrade Vilas BoasI
I Department of Dentistry, Metropolitan Union of Education and Culture – Lauro de Freitas – BA – Brazil
ABSTRACT
Introduction: The ceramic laminates gained space in Esthetic Dentistry due to conservative preparations, excellent optical properties, durability, and longevity. Additionally, the use of digital planning to assist the smile reconstruction also allows the outcome predictability. Objective: To present and discuss a clinical case of smile reconstruction with ceramic laminates using as esthetic planning the Digital Smile Design. Case report: 25-year-old female reported dissatisfaction with her smile. After clinical and radiographic exam, Digital Smile Design was the method chosen, which enabled to verify the need for clinical crown augmentation and to construct the porcelain laminates for the maxillary anterior teeth. After the mock-up and the patient's agreement, the treatment was performed. Results: A significant improvement in the esthetics of the planned smile, with approval of the patient was obtained. Conclusion: The digital planning for smile reconstruction with ceramic laminates proved to be an excellent tool to aid in this choice of treatment.
Keywords: treatment plan; dental laminates; dental esthetic.
Introduction
The cosmetic for humans is a highly subjective concept, since it is related to social, cultural, and psychological factors which change as a function of time, the values of life, and age of the individual 7.
The anterior teeth play a fundamental role in the esthetics of the face and, therefore, are highly valued by patients who want to whiten, increase, improve the anatomy and/or their position in the search for a smile considered more natural and harmonious 6.
The current trend is the changes in the smile be performed with minimum wear of healthy tooth structure 13. The laminates have a conservative preparation and have stood out due to their excellent optical properties, material durability, longevity, and outcome predictability. However, these properties and clinical conditions are obtained when there is a correct diagnosis associated with good planning and construction of the prosthetic pieces 3.
Additionally, the assessment of the patient's expectations and understanding of the potential therapeutic approaches are essential before starting any planning. Thus, one can consider planning as the most important stage of restorative treatment, as it gives opportunity for the predictability of the treatment and its results, allowing that possible failures are minimized 1,2.
Coachman et al.5 featured the Digital Smile Design (DSD) as a new and powerful tool for planning in cosmetic dentistry. It comprises the use of digital tools on intraoral and face photos of the patient, to assess better the esthetic relationship between the teeth, the gums, the smile, and face. For the authors, the proposed DSD protocol aims to improve the aesthetic diagnosis, interdisciplinary communication, critical aesthetic analysis of the treatment, management of expectations, education, and motivation.
Another important factor for the success of the treatment is the choice of the ceramic to be used. Currently, the new ceramic systems have higher esthetic and greater resistance, they are reinforced with leucite and lithium disilicate, enabling the performance of minimally invasive ceramic veneers and thin thickness 3,10 – i.e., use of thin ceramic (0.1 to 0.7mm thick) over the tooth structure with minimal or no wear, without interfering in the material strength 9,11. Ideally, the chosen ceramic system also presents the possibility of a partial stratification with veneering porcelain that reproduce much amount of details in the incisal area of anterior teeth, and may be 50% made up and 50% stratified, depending on the needs to be played 8.
The adhesive cementation, used in this type of procedure is the most critical phase of the entire protocol, presenting details that must be strictly followed in order to reach proper adhesion. Details on the preparation of the prosthetic piece and the dental substrate, cement applied evenly, and thickness of the adhesive and the applied cement are factors that directly influence on the outcome 4,5.
Considering the above, this study aimed to present and discuss a case of smile reconstruction with ceramic laminates using as aesthetic planning the Digital Smile Design.
Case report
A 25-year-old female search treatment at the Post-graduate clinics of Operative Dentistry in the Center of Dental Studies of Bahia (CEBEO) reporting dissatisfaction of her smile and desiring improving the esthetic of the maxillary incisors.
In clinical and radiographic examinations, we evaluated the facial features, the smile, the gingival contour, and dental characteristics. With the permission of the patient, the proposed method of choice for treatment planning was Digital Smile Design.
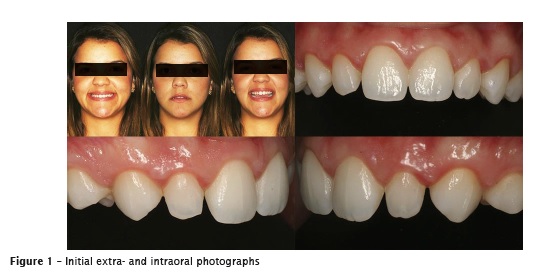
The face and intraoral photographs of the patient was taken (figure 1) to enable the digital planning.
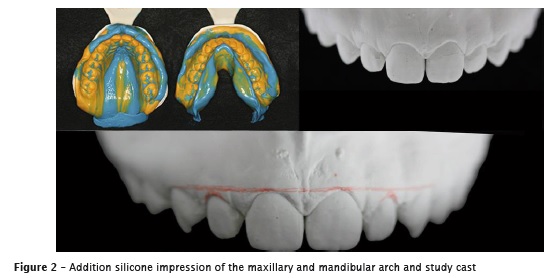
At that same appointment, the impression (figure 2) was taken with the aid of addition silicone Express (3M ESPE, Germany). The occlusal record was obtained with Occlufast (Zhermack, Italy).
Two lines are placed on the center of the slide at an angle of 90 degrees between them, and the facial photo is placed behind the lines (figure 3A). These lines are transferred to the smile region, allowing a comparative analysis between tooth and face. Also, we traced lines of the upper and lower lips and the smile line (figure 3B). The digital ruler is calibrated on the picture, allowing the measurement of important relationships evidenced by the drawings (figures 3C and 3D).

During planning, it was possible to verify the need of clinical crown augmentation and inclusion of canines in the treatment, to improve the smile harmony. Thus, the waxing-up (figures 4A and 4B) was made based on the digital planning obtained after the approval of the patient and subsequent realization of a template (figure 4C) with condensation silicone Express (3M ESPE, Germany) to obtain the mock-up (figure 4D) with bis-acryl resin Protemp, shade A2 (3M ESPE, Germany).

Based on the patient's complaint and after the examination analyses (clinical, radiographic and photographic), the proposed treatment planning was ceramic laminates on teeth #13, #12, #11, #21, #22, and #23, with the ceramic system IPS e.max – lithium disilicate (Ivoclar Vivadent, Leichtenstein).
Minimally invasive tooth preparation was performed with the aid of diamond point #3216 (KG SORENSEN, Brazil) by removing only the retention areas. Aluminum oxide discs (Cosmedent, Brazil) were used for prepare polishing, followed by felt disc and aluminum oxide paste (Cosmedent, Brazil). We emphasized that due to the minimally invasive preparation, no provisional crowns were needed.
The maxillary impression for obtaining the working cast was performed with addition silicone Express (3M ESPE, Germany) through one-step technique associated with gingival displacement with double wires (wires #000 and #00 – Ultrapack, Ultradent, USA). The wire #000 was kept inside the gingival sulcus, while the wire #00 was removed. The shade selection was executed with VITA 3D scale; the shade chosen was 0M3.
The laminates were constructed in the laboratory (figure 5), and the patient returned for the proof of the pieces with the aid of the try-in paste Variolink Veneer Try-In (Ivoclar Vivadent, Leichtenstein). After the color selection of the cement, the laminates were washed to remove the try-in paste. Next, the laminates were etched with 10% hydrofluoric acid for 20 seconds. The laminates were copiously washed with water/air jets to remove the residues of the acid etching and dried. Silane agent was applied for 1 minute, then, the laminates were dried with air jet, and an adhesive agent was applied.

Prior to the cementation of the laminates, the teeth underwent relative isolation with cotton rolls and a retractor wire #000 (Ultrapack, Ultradent, USA) was inserted into the gingival sulcus of the teeth. The teeth were cleaned with pumice and water with the aid of a Robinson brush at low speed. Then, the teeth were etched with 37% phosphoric acid for 30 seconds, washed and dried with water/air jet. The adhesive agent was applied without light-curing.
The cementation of the laminates was performed individually, with light-cured resin cement Variolink Veneer (Ivoclar Vivadent, Leichtenstein). The cement was mixed, applied onto the laminates, which were put into position. Prior to the light-curing for 40 seconds, all cement excess was removed with the aid of size 1/2 Suprafil spatula and dental floss.
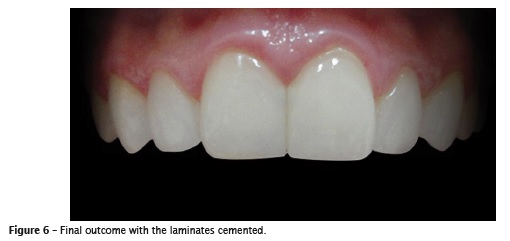
The final outcome exhibited that all esthetic parameters and patient's and dentist's expectations were met (figure 6).
Discussion
To obtain increasingly predictable results in the use of ceramic laminates, it is necessary to plan before executing. Higashi et al. 7 affirmed that in an aesthetic analysis of anterior teeth, there are a lot of information to be observed, and these can hardly be recorded during the first clinic visit. Obtaining photographs at different angles can help the professional to analyze calmly the aesthetic details in the absence of the patient, besides being a very interesting way to convey to the patient the information on the clinical problems found, as in the case presented here.
The Digital Smile Design, proposed by Coachman et al. 5 and used in this present clinical case, put digital photos together to facilitate the analysis of facial and dental proportions of patients with the advantage of planning a given treatment even when the patient is not in the office. After examination and treatment of the pictures, a digital image is created that can be considered the final design of the smile, which, together with the patient, can be analyzed and discussed and, then, approved. Another DSD advantage when compared with other methods, it is the possibility of monitoring before, during, and after treatment.
One can also consider the marketing that planning and communication with the team provides. As an example, the guided aesthetic diagnostic wax-up will be an important reference for all surgical, orthodontic, and restorative procedures. Several templates can be produced on this wax-up to assist such steps. Thus, the predictability of a favorable outcome becomes much higher 5.
Rodrigues et al. 14 evaluated in their study the perception of dentists and lay people on variations in aesthetic smile standards. It was concluded that dentists and lay people have different opinions when evaluating the same smiles; thus, the decisions of aesthetic treatments should be taken together. The presence of small deviations can be accepted aesthetically, but not all variations have the same degree of aesthetic acceptance. In the clinical case described here, the patient actively participated in the process, issuing her opinion and approval of the results, facilitating the desired outcome of the smile esthetics.
Considering the material chosen for the, Soares et al. 15 affirmed that with the development of dental materials, ceramics have become a great option due to the ability to reproduce the appearance of natural teeth and present similar biomechanical behavior of the enamel, allowing minimally invasive preparations
Mondelli et al. 12 claim that the selection of the ceramic should be based on the full knowledge of the professional about the system and sent to a laboratory with equipment and specialized technicians used with the chosen ceramics.
According to Kina et al. 9, the correct choice of the ceramics to indicate the laminates is the capacity of receiving etching. The leucite- (IPS Empress) and lithium disilicate-reinforced (IPS Empress 2, EMAX) systems have smaller contraction than the conventional ceramics, with better adaptation and optical quality, smaller resistance to fracture, and they can be adhered to the dental structures because the ability to be etched and silanized.
However, Rodrigues et al. 14emphasize the need for an enlightening conversation with the patient about the planning. It should be noted that it is a design in digital media and there are clinical limitations for the implementation of the proposed treatment. The accurate documentation is a prerequisite to ensure that the patient understands the limitations of the cosmetic procedure.
The digital planning is not a photo manipulation with perfect finish, and the drawings superimposed on the picture should be evident, as the proposed objective is just a result simulation without creating expectations in the patient in relation to an identical reproduction of digital planning. The use of more sophisticated programs of image manipulation could create an unattainable reality, considering the clinical and functional individualities of the treatment in question 14.
Conclusion
Given the above, DSD has proved to be a very effective tool to give predictability of what was to come in the smile reconstruction. The patient's opinion was taken into consideration and she approved the treatment planning, which made the process much more communicative, predictable and personalized. At the end of treatment, the main objectives were achieved by returning a more harmonious smile for the patient, who complained of her smile with childish features.
References
1. Araújo EM, Baratieri LN, Monteiro JRS, Vieira LCC, Andrade MAC. Direct adhesive restoration of anterior teeth: part 1. Fundamentals of excellence. Pract Proced Aesthet Dent. 2003;15(3):223-40. [ Links ]
2. Baratieri LN. Estética: restaurações adesivas diretas em dentes anteriores fraturados. 2ª ed. São Paulo: Santos; 1998. p. 397.
3. Cardoso PC, Cardoso LC, Decurcio RA, Monteiro LJE. Restabelecimento estético funcional com laminados cerâmicos. Rev Odontol Bras Central. 2011;20(52):88-93.
4. Cherukara GP, Seymour KG, Samarawickrama DY, Zou L. A study into the variations in the labial reduction of teeth prepared to receive porcelain veneers – a comparison of three clinical techniques. Dent J. 2002;192(7):401-4.
5. Coachman C, Calamita M, Schayder A. Digital Smile Design: uma ferramenta para planejamento e comunicação em odontologia estética. DICAS. 2012;1(2):36-41.
6. Gonzalez MR, Ritto FP, Lacerda RAS, Sampaio HR, Monnerat AF, Dias-Pinto B. Falhas em restaurações com facetas laminadas: uma revisão de literatura de 20 anos. Rev Bras Odontol. 2011;68(2):238-43.
7. Higashi C, Gomes JC, Kina S, Andrade OS, Hirata R. Planejamento estético em dentes anteriores. In: Mello AT, Miyashita E, editores. Odontologia estética – planejamento e técnica. 1. ed. São Paulo: Artes Médicas; 2006. p. 139-54.
8. Higashi C, Reggiani RD, Kina S, Scopin O, Hirata R. Cerâmicas em dentes anteriores: parte I – indicações clínicas dos sistemas cerâmicos. Clínica – Int J Braz Dent. 2006;2(1):22-31.
9. Kina S, Rocha EP, Andrade OS, Celestrino M. Laminados cerâmicos – odontologia estética: o estado da arte. São Paulo: Santos; 2004.
10. Magne P, Belser UC. Novel porcelain laminate preparation approach driven by diagnostic mockup. J Esthet Restor Dent. 2004;1(16):7-16.
11. Marson FC, Kina S. Restabelecimento estético com laminados cerâmicos. Rev Dental Press Estét. 2010;7(3):76-86.
12. Mondelli RFL, Coneglian EAC, Mondelli J. Reabilitação estética do sorriso com facetas indiretas de porcelana. Biodonto. 2003;1(5).
13. Peumans M, Van Meerbeek B, Lambrechts P, Vanherle G. Porcelain veneers: a review of the literature. J Dent. 2000;28(3):163-77.
14. Rodrigues C, Loffredo L, Candido MS, Oliveira- Junior O. Influência de variações das normas estéticas na atratividade do sorriso. Rev Gaúcha Odontol. 2010;58(3):307-11.
15. Soares PV, Zeola LF, Souza PG, Pereira FA, Milito GA, Machado AC. Reabilitação estética do sorriso com facetas cerâmicas reforçadas por dissilicato de lítio. Rev Odontol Bras Central. 2012;21(58):538-43.
 Corresponding author:
Corresponding author:
Giulian Lennon de Macêdo
Rua Maceió, s/ n.º
Condomínio Bela Vista
Área 1, Bloco 4, ap. 203 – km 25
Jardim Eldorado
CEP 43700-000
Simões Filho – BA – Brasil
E-mail: giulian.lennon@gmail.com
Received for publication: November 7, 2015
Accepted for publication: April 5, 2016
