










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRSBO (Online)
versão On-line ISSN 1984-5685
RSBO (Online) vol.13 no.2 Joinville Abr./Jun. 2016
CASE REPORT ARTICLE
Impacted tooth associated with dentigerous cyst and compound odontoma – case report
Letícia de Souza MoraesI; Ruth Peggy BravoI; João Gilberto DudaI; Juliana Feltrin de SouzaII; Estela Maris LossoI; Melissa Rodrigues de AraujoI
I Positivo University – Curitiba – PR – Brazil
II Federal University of Paraná – Curitiba – PR – Brazil
ABSTRACT
Introduction: The dentigerous cyst is a benign cyst associated with the development of odontogenic epithelium that covers the crown of impacted teeth. These are prevalent in the first three decades of life, reaching more often Caucasian males. Odontomas are hamartomas affecting the dental tissues, which can be divided into compound and complex odontoma. Odontoma affects children and young adults of both sexes, with a predilection for jaw bone. Case report: A 12-yearold boy attended the Pediatric Dentistry Clinic of Positivo University, complaining of pain in right parasymphysis region. The panoramic radiograph showed an impacted tooth (#43) located in base of the jaw below the apex of the teeth #31 to #42, with increased follicle. A radiopaque mass with small fragments of approximately 1 cm, located at the apex of the teeth #83 and #84 was seen. The patient underwent surgery under general anesthesia to remove the impacted tooth and radiopaque injury. Histopathological analysis of the dental follicle was compatible with dentigerous cyst and dental fragments were diagnosed as compound odontoma. The postoperative was uneventful, four months after the surgery the patient began orthodontic treatment for traction of tooth #44. Conclusion: Both lesions, dentigerous cyst and compound odontoma have favorable prognosis and low recurrence rate, but must be removed to maintain the integrity of the stomatognathic system. In this case was important the inter-relationship between dental specialties for the treatment of the patient.
Keywords: dentigerous cyst; odontoma compound; impacted tooth.
Introduction
Odontomas and dentigerous cysts are common lesions with known growth pattern 18. Cysts are pathological cavities, enclosed by the epithelium, which may contain liquid, solid or semi-solid material. Cysts are chronic, asymptomat ic, slow-growing lesions. In most cases, they are detected in routine radiographic examination 7. The dentigerous cyst is a benign odontogenic developmental cyst and originates from the accumulation of fluid between the enamel organ and the underlying dental crown, usually located in impacted, unerupted teeth or teeth with late eruption 11. The dentigerous cyst is the most common odontogenic developmental cyst and represents about 20% of all cysts surrounded by epithelium that affects the maxillary bones 12. The presence of dentigerous appears with a frequency of 1.44 in 100 unerupted teeth 14. The most affected teeth are the mandibular third molars, maxillary canines, and mandibular premolars 24. Impacted canines, when associated with dentigerous cyst during its eruption path suffer displacement and may cause root resorption of adjacent teeth 22. The incisors are in 12% of cases affected by root resorption caused by the included canine associated with dentigerous cyst 25.
Odontoma s a re common odontog eni c tumors, considered developmental abnormalities, hamar tomas composed of epithelial and mesenchymal tissue when fully formed, they are presented primarily as enamel and dentin, with a minor amount of pulp and cementum 5. The World Health Organization (WHO) classified into two main types: complex and compound. The compound odontomas arise from an excessive proliferation of the dental lamina forming structures similar to denticles 10. The most accepted etiology relates to trauma, infection, or pressure on the site of formation, causing changes of tooth development 8. They are discovered in routine radiographs because they are asymptomatic. The treatment is the total surgical excision with a favorable prognosis, having a good bone repair, and rare cases of recurrence 21.
This study aimed to report a case of occurrence of dentigerous cyst and composed odontoma, emphasizing the treatment performed and the importance of the interrelationship among dental specialties.
Case report
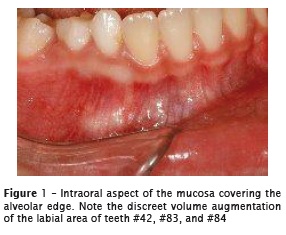
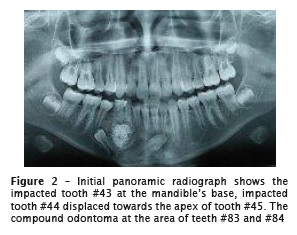
A 12-year-old boy was referred by a practice private dentist to the Pediatric Dentistry Clinics of the Positivo University, with a panoramic radiograph and chief compliant of pain in the right mandibular parasymphysis area. At the physical examination, we observed a discreet volume augmentation in the labial area of teeth #42, #83, and #84. The gingiva was sound, plain, and shiny with color similar to that of the adjacent oral mucosa (figure 1). The teeth had good general health. The panoramic radiographic revealed an impacted tooth (#43) located at the mandible's base below the apexes of the teeth #31 to #42, with increasing of the dental follicle. A radiopaque mass with small fragments of approximately 1 cm, located at the apex of the teeth #83 and #84 was seen. The tooth #44 was impacted and displaced towards the apex of #45 (figure 2).
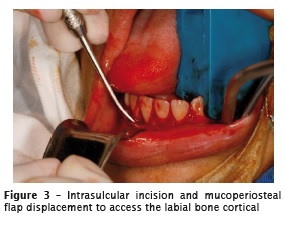
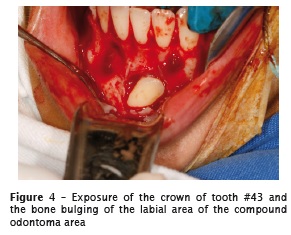
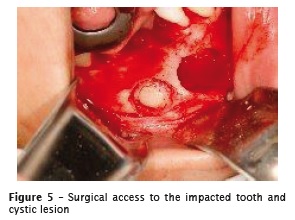
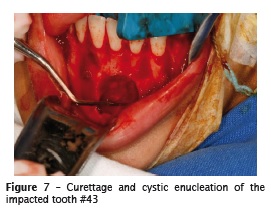
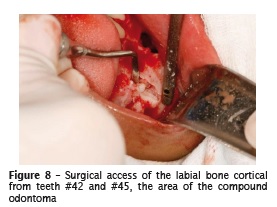
All pre-surgical tests were within the normality. The boy was submitted to the surgery under general anesthesia to remove the impacted tooth and the radiopaque lesion. For this purpose, intrasulcular and oblique incisions from tooth #33 to #46, followed by mucoperiosteal displacement (figures 3 and 4) and osteotomy on the area to locate the crown of the tooth #43 (figure 5). The impacted tooth #43 was extracted followed by curettage and enucleation (figures 6 and 7). At the area of compound odontoma, the surgical access was through the labial bone cortical, from teeth #42 to #45 (figure 8), followed by the removal of the tooth fragments (figure 9).


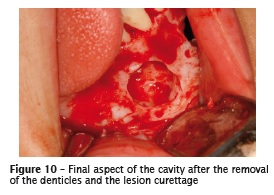
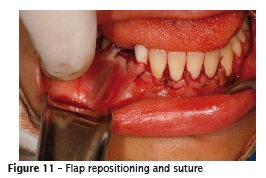
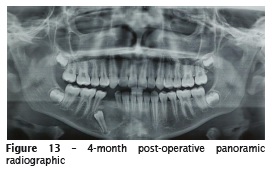
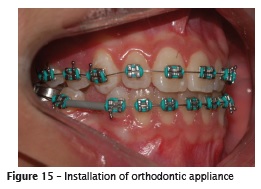
Then, the site was curetted (figure 10), and the flap was repositioned and sutured (figure 11). The material removed by curettage was sent to histopathological analysis (figure 12). The result was compatible with dentigerous cyst and the tooth fragments with compound odontoma. The four-month post-operative period was uneventful (figures 13 and 14). Ten months after the surgery, the child started the orthodontic treatment for traction of tooth #44 (figures 15 and 16).



Discussion
Delays in tooth eruption may be related to the presence of local or systemic changes. Local changes are lack of space in the arch, presence of supernumerary teeth, cysts, tumors 27. The systemic changes are associated with craniofacial syndromes, hereditary factors, and endocrine disorders 11. According to this case report, the teeth #44 and #43 were delayed in eruption, because of prolonged retention of teeth #83 and #84 because they were affected by tumor lesion, compound odontoma and the tooth #43 engaged in a dentigerous cyst.
Both injuries affect the mandibular symphysis region, but not associated, with each one located in different anatomic regions, only close to each other, which is rarely described in the literature. When such injuries occur in the same anatomical space, they are called mixed lesions, as described by Costa et al. 5. The literature explains the development of mixed injuries. Some authors advocate the genetic mutation theory2, the ability of the odontogenic epithelium undergoes morphological and histological differences for the formation of a mixed injury3. Others defend the thesis of the secondary development of injury from a pre-existing lesion 1. In a classic study of literature evaluated 351 cases of odontomas: 27.6% of cases were involved with dentigerous 9.
The dentigerous cysts and odontomas are lesions with clinical and radiographic features widely described in the literature 6. Due to present asymptomatic evolution, these injuries are found in routine radiographs, or in those for other purposes, such as research on the late eruption of permanent teeth 23. The dentigerous cyst is the most common cyst that affects the jaw bones, and in most cases is associated with the crown of unerupted teeth, with predilection for affecting the region of third molars and canines 4. In this case report, the cystic lesion affected the impacted right mandibular canine. The dentigerous cyst has as clinical features: slow and asymptomatic growth and may cause displacement of the teeth and adjacent structures, facial deformity and root resorption of teeth involved. Commonly, the dentigerous cyst has a characteristic radiolucent unilocular radiographic image, but may have multilocular image, when it reaches great proportions 26. This information corroborates the case report, in which it was observed a radiolucent unilocular image and displacement of tooth #43. Odontomas are odontogenic tumors that most affect the population 28, and 67% of tumors in maxillary bones are classified as complex odontoma and compound odontoma 20. According to Oliveira et al. 16, the frequency with compound odontoma occurs in 9% to 37% of cases; and complex odontoma 5% to 30% of cases. In this case report, the patient exhibited a compound odontoma involving the teeth #83 and #84. The compound odontoma consists of several rudimentary denticle structures 17. It frequently reaches the maxilla , unlikely this case report in which it affects the mandible. Clinically, odontomas are asymptomatic, of slow and limited growth, with the potential to evolve into complex odontomas often associated with unerupted permanent teeth. Radiographically, the odontoma has centralized radiopaque mineralized structures similar to teeth, circumscribed by a defined radiolucent halo 22, characteristics observed in the radiograph of the case.
The treatment of choice for cystic lesions depends on several features. The decision of which technique is used will depend on the size of the cyst and the proximity to important anatomical structures. The cystic enucleation is the therapy of choice for small sizes of injuries that consists of surgical excision of the lesion and the involved tooth without compromising adjacent structures; it is a definitive treatment, which provides more information to complete the histopathology result 4. Marsupialization is another treatment option for dentigerous cyst; however, it is indicated for larger lesions with involvement of important anatomical structures, the technique uses devices to decompress the injury as a result of intracystic decreasing 13. In the case described here, we used the surgical cystic enucleation, in which tooth #43 was extracted along with the lesion.
Once diagnosed compound odontoma, it must be removed. The recommended treatment is surgical enucleation, followed by curettage of the lesion, to minimize recurrence rates 19. In the case report here, the compound odontoma was removed completely. The prognosis for both dentigerous cyst and compound odontoma is favorable, with low recurrence rate 5.
Conclusion
The interrelationship between dental specialties pediatric dentistry, oral and maxillofacial surgery, and orthodontics was of great importance for the early diagnosis and treatment of injuries. The multidisciplinary approach of the specialties provided an effective treatment, seeking to rehabilitate the physiology, aesthetics, and masticatory function of the patient.
References
1. Alvarez SG, Jimenez FM, Gómez FJT, Vecino FJA, Fernadez CS. Calcifying odontogenic cyst associated with complex odontoma: case report and review of the literature. Med Oral Patol Oral Cir Bucal 2005;10:243-7. [ Links ]
2. Basile JR, Klene C, Lin YL. Calcifying odontogenic cyst with odontogenic keratocyst: a case report and review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010;109(4):40-5.
3. Bernardes VF, Lacerda JC, Aguiar MC, Gomez RS. Calcifying odontogenic cyst associated with an orthokeratinized odontogenic cyst. Head Neck Pathol 2008;2(4):324-7.
4. Caliento R, Mannarino FS, Hochuli-Viera E. Cisto dentígero: modalidades de tratamento. Rev Odontol UNESP. 2013;42(6):458-62.
5. Costa DD, Marques Neto JA, Freitas DJSM, Andrade EL, Lima RG, Freitas CE. Cisto dentígero associado ao odontoma composto: lesão mista. Clipe Odonto. 2013;5(1):25-30.
6. Dantas RMX, Costa DD, Toledo IC, Oliveira Júnior JATB, Bonfim RT, Almeida de Azevedo R. Cisto dentígero associado a dente ectópico – relato de caso. Academia Tiradentes de Odontologia. 2012;8: 952-62.
7. Freitas A, Rosa JE, Souza IF. Radiologia odontológica. 6. ed. São Paulo: Artes Médicas; 2004.
8. Güngörmüş M, Yolcu Ü, Aras MH, Halicioğlu K. Simultaneous occurence of compound odontoma and arrested root formation as developmental disturbances after maxillofacial trauma: a case report. Med Oral Patol Oral Cir Bucal. 2010;15(2):398-400.
9. Kaugars GE, Miller ME, Abbey LM. Odontomas. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontology. 1989(67):172-6.
10. Lukes SM, Wachter KM. Compound odontoma: a case study. The Journal of a Dental Hygiene. 2003;77(1):47-9.
11. Machado LM, Valerio CS, Pacheco W, Maia BF, Capistrano HM. Cisto dentígero associado a canino: o sucesso de uma abordagem clínico-cirúrgica. Rev Odontol Bras Central. 2014;23(64):35-9.
12. Meningaud JP, Oprean N, Pitak-Arnnop P, Bertrand JC. Odontogenic cysts: a clinical study of 695 cases. J Oral Sci. 2006;48(2):59-62.
13. Montevecchi M, Checchi V, Bonetti GA. Management of a deeply impacted mandibular third molar and associated large dentigerous cyst to avoid nerve injury and improve periodontal healing: case report. J Can Dent Assoc. 2012;78(c59):1/6-6/6.
14. Mourshed F. Roentgenographic study of dentigerous cysts: III. Analysis of 180 cases. Oral Surg Oral Med Oral Pathol. 1964;18:66-73.
15. Neville BW, Damm DD, Allen CM, Bouquot JE. Patologia oral e maxilofacial. 3. ed. Rio de Janeiro: Elsevier; 2009.
16. Oliveira BH, Campos V, Marçãl S. Compound odontoma – diagnosis and treatment: three case reports. American Academy of Pediatric Dentistry. 2001;23(2):151-7.
17. Regezi JÁ, Sciubba JJ. Patologia bucal: correlações clínico-patológicas. 3. ed. Rio de Janeiro: Guanabara Koogan; 2000.
18. Sales MA, Cavalcanti MG. Complex odontoma associated with dentigerous cyst in maxillary sinus: case report and computed tomography features. Dentomaxillofacial Radiology. 2009;38:48-52.
19. Santos MESM, Silva ARBL, Florêncio AG, Silva UH. Odontoma como fator de retenção dentária: relato de casos clínicos. Rev Cir Traumatol Buco- Maxilo. 2009;10(2):25-30.
20. Santos DLM, Dantas-Neta DB, Gomes LCL, Moraes SS, Lopes MCA, Barros SSLV. Large complex odontoma with facial asymmetry: a case report. Rev Cir Traumatol Buco-Maxilo-Fac. 2012;12(4):39-44.
21. Serra-Serra G, Berini-Aytés L, Gay-Escoda C. Erupted odontomas: a report of three cases and review of the literature. Med Oral Patol Oral Cir Bucal. 2009;14(6):299-303.
22. Silva FWGP, Queiroz AM, Borsatto MC, Nelson- Filho P. Principais tumores odontogênicos que podem acometer a cavidade bucal de crianças. Revista de Odontologia da Universidade Cidade de São Paulo. 2007;19(2):181-7.
23. Smith JL, Kellman RM. Dentigerous cyst presenting as a head and neck infections. Otolaryngol Head Neck Surg. 2005;133(2):715-7.
24. Takagi S, Koyama S. Guided eruption of an impacted second premolar associated with a dentigerous cyst in the maxillary sinus of a 6- year-old child. J Oral Maxillofac Surg. 1998;56(2): 237-9.
25. Turner JP, Bedi R. Combined orthodontic and restorative management of a case of bilateral ectopic canines and resorbed central incisors. Br Dent. 1996;180(2):67-72.
26. Vaz LGM, Rodrigues MTV, Ferreira Júnior O. Cisto dentígero: características clínicas, radiográficas e critérios para o plano de tratamento. RGO. 2010;(58):127-30.
27. Vianna AP, Monini AC, Machado AW, Gandini Júnior LG. Alternativa de tratamento simplificado e integrado da retenção intraóssea de incisivo central superior, associada a odontoma: relato de caso. Rev Odontol Bras Central 2012;21(56): 484-8.
28. Yadav M, Godge P, Meghana SM, Kulkarni SR. Compound odontoma. Contemporary Clinical Dentistry. 2012;(3):S13-S15.
 Corresponding author:
Corresponding author:
Melissa Rodrigues de Araujo
Mestrado em Odontologia Clínica
Universidade Positivo
Rua Professor Pedro Viriato Parigot de Souza, n. 5.300
Campo Comprido
CEP 81280-330 – Curitiba – PR – Brasil
E-mail: melissararaujo@hotmail.com
Received for publication: February 14, 2016
Accepted for publication: April 15, 2016
