










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRSBO (Online)
versão On-line ISSN 1984-5685
RSBO (Online) vol.13 no.3 Joinville Jul./Set. 2016
ORIGINAL RESEARCH ARTICLE
Bond strength of resin cements to leucite-reinforced ceramics: part 2 – after one-year aging in water
Rubens Nazareno GarciaI,II; Reinaldo Francisco do NascimentoIII; Ana Cristina Rocha GomesIII; João Augusto Coutinho GarciaII; Luiz Carlos Machado MiguelI; Peter Clayton MoonIV; Shélen Xavier FernandesI
I Department of Dentistry, University of the Region of Joinville – Joinville – SC – Brazil
II School of Dentistry, University of Itajai Valley – Itajai – SC – Brazil
III RPD Dental Laboratory – Joinville – SC – Brazil
IV Department of General Practice, School of Dentistry, Virginia Commonwealth University – Richmond – VA – USA
ABSTRACT
Objective: The aim of this study was to compare the shear bond strength (SBS) of two resin cements bonded to four leucite-reinforced ceramics after one week and one year of aging. Material and methods: Forty ceramic blocks (4 mm wide, 14 mm length, and 2 mm thick) were used (1 week) and reused at the back side (1 year). The blocks were abraded with aluminum oxide (90 μm) and randomly divided into eight groups for each time. Two dual resin cements (RelyX ARC and RelyX U200 self-adhesive, 3M ESPE) were bonded to ceramics Creapress (CRE – Creation / Klema), Finesse All-Ceramic (FIN – Dentsply / Ceramco), IPS Empress Esthetic (IEE – Ivoclar Vivadent) and Vita PM9 (PM9-Vita). For each resin, time, and ceramic block, after applications of the 10% hydrofluoric acid (for 1 min) and silane, 3 Tygon cut tubes were positioned over each block and filled in with the resin cements (light-cured for 40 s). The tubing molds were removed to expose the bond specimens as cylinders (area=0.38 mm2) stored in relative humidity at 24±2°C for one week and at 37±2°C for one year. All bonds were tested in an Instron in shear (applied of the base cylinder with a thin wire - 0.25 mm) at speed of 0.5 mm/min, until failure. Results: The results were analyzed by ANOVA (resin cements, ceramic systems, and time) and Tukey test (p<0.05) for rank ordering of SBS. The FIN and IEE ceramics did not show significant SBS decreasing on aging with U200. The mean SBS decreasing for all the ceramics was 36% with ARC and 14% with U200 cement. Conclusion: The SBS of ARC cement were significantly lower for all ceramics with aging than that of U200 cement. The SBS of ARC cement was also weakened by aging. FIN ceramic + U200 cement proved to be the most stable and strongest bond strength, and PM9+ARC cement proved to be the weakest bond strength with low stability.
Keywords: ceramics; resin cements; shear strength.
Introduction
The growing demand for aesthetic in dentistry led researchers and manufacturers to research and develop the most diverse materials that meet this requirement. From this research and development, arose materials such as restoration composites, dental adhesive systems, dental ceramics, and resin cements that year after year have been improved, meanly regarding to its mechanical and aesthetic properties 1,3.
The success of indirect restorations, single crowns or retainers of fixed partial dentures, depend on a correct diagnosis and planning, proper design of preparations and huge clinical knowledge, in addition to the right choice of the cementing agent and its cementing technique. The retention of an indirect restoration can be made by conventional cementation, which mainly involves mainly the zinc phosphate cements and glass ionomer cements. However, an adhesive cementation is necessary for most of the dental ceramics, especially for leucitereinforced ceramic 2,16.
The search for a simpler adhesive dentistry brought the development of a new type of resin cement, so-called self-adhesive. This material was designed to overcome some limitations of conventional cements (zinc phosphate, zinc polycarboxylate, and glass ionomer), as well as meet in a single product some favorable characteristics of these different cements. The sensitivity of the adhesive technique was also simplified on the selfadhesive cement, which is presented in a single step, eliminating the previous application of an adhesive or another pre-treatment of the tooth 8,13.
The aim of this study was to compare the shear bond strength (SBS) of two resin cements bonded to four leucite-reinforced ceramics at one week and one year of aging. The null hypothesis tested was that there was no statistical difference in shear bond strength between resin cements and leucitereinforced ceramics after aging.
Material and methods
Forty leucite-reinforced ceramic blocks (4 mm wide, 14 mm length and 2 mm thick) were constructed in the hot pressing technique using Creapress (CRE – Creation/Klema – Batch #8746), Finesse All-Ceramic (FIN – Dentsply/Ceramco – Batch # 2887), IPS Empress Esthetic (IEE – Ivoclar Vivadent – Batch #0305) and Vita PM9 (PM9 – Vita – Batch #17290). The blocks were used (1 week) / reused at the back side (1 year), the samples were abraded with aluminum oxide (90 μm/2,5 bar/10 mm distance), and divided into eight groups (n=5) for each period of testing (1 week/1 year).
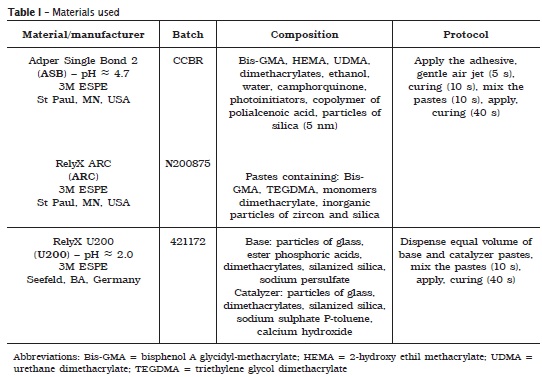
For all groups and in each sample, after application of the 10% hydrofluoric acid for 1 min (Condac Porcelana, FGM, Joinville, SC, Brazil – Batch #40511), rinsed for 1 min, airdried for 1 min, followed by the application of the silane coupling agent (Prosil, FGM, Joinville, SC, Brazil – Batch #130411) for 1 min and then air-dried for 30 s – according to Shimada et al. 17– three Tygon tubings (TYG-030, Saint-Gobain Performance Plastic, Maime Lakes, FL, USA) were positioned over the samples and filled in with the resin cements RelyX ARC or RelyX U200, and light-cured for 40 s (Led Radii-cal 1.200 mW/cm2, SDI, Bayswater, VI, Australia).
The materials and adhesive protocols are listed in Table I and the experimental groups were: 1 ASB+ARC+CRE; 2ASB+ARC+FIN; 3ASB+ARC+IEE; 4 ASB+ARC+PM9; 5 U200+CRE; 6 U200+FIN; 7 U200+IEE; 8 U200+PM9.
Afterwards, the tubing molds were removed to expose the specimens in format of cylinders (area: 0.38 mm2), which were stored in relative humidity at 24±2°C for one week. The oneyear specimens were stored in water at 37±2°C. After these respective periods, each sample was attached to the universal testing machine Instron (model TTC, Canton, MA, USA) and the specimens were tested in shear (applied at the base of the specimen/cylinder with a thin wire - 0.2 mm) at speed of 0.5 mm/min, until failure. The results were analyzed by ANOVA (resin cements, ceramic systems and time) and Tukey test (p<0.05) for rank ordering of SBS.
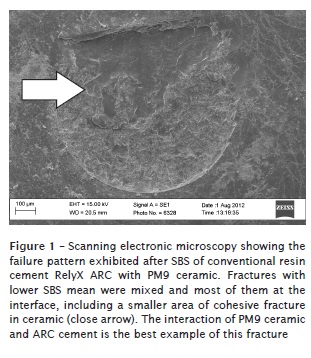
The specimens were mounted into a n aluminum base, metal i zed with gold, and examined in scanning electronic microscope (Carl Zeiss AG – EVO® 50 Series, Oberkochen, Germany). Photomicrographies of representative areas were obtained to evaluate the fracture pattern that was classified in adhesive, cohesive (either in ceramic or in cement), and/or mixed.
Results
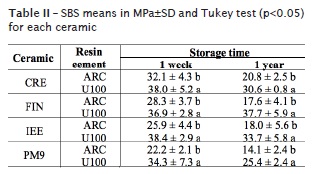
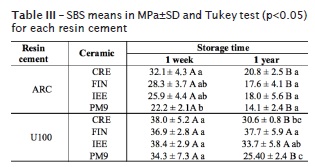
The ANOVA showed significant differences (p<0.001) for the two cements, for the ceramic systems, and storage time. To investigate the differences between means of the ceramic systems, the Tukey test was applied (p<0.05). The U200 cement SBS were significantly higher than that of the ARC cement, for one week and one-year storage time. The interaction of the U200 cement and the ceramics FIN and IEE did not decrease the SBS after one-year aging; also there was a 36% decrease in the SBS for ARC, and 14% decrease for U200. FIN ceramic + U200 cement proved to be the most stable and strongest bond strength, and PM9 + ARC cement proved the weakest bond strength with low stability (tables II and III).
Discussion
The technological evolution and the search of patients by imperceptible restorations have promoted the development of materials that connect mechanical and aesthetic properties in the manufacturing of metal-free restorations. Thus, materials such as ceramics and resin cements are being more frequently used in dental rehabilitations in order to promote a final aesthetically result more natural and closer to the tooth structure 2-4,9,12.
This study is part of the Ceramics Project, which is the second part of the study held by Garcia et al. 6, and had as objective to compare the shear bond strength of two resin cements with four leucite-reinforced ceramics, now including the data of storage in distilled water for one year. The null hypothesis tested was rejected, because there were statistical significant differences in shear bond strength between resin cements and among the leucite-reinforced ceramics after aging.
The methodology proposed in both studies was the microshear bond strength introduced in the literature initially by Shimada et al. 17. This type of mechanical test solves problems related to tension spreads in the bond interface over large areas. It presents the advantage that several specimens can be obtained from a single sample without need to cut it, an easier and cheaper solution in comparison to the microtensile test, when samples need to be cut to obtain the specimens.
The resin cements have many advantages when compared to conventional powder/liquid cements: better retention, minimum solubility in the oral cavity, lower microleakage, and acceptable biocompatibility. But conventional resin cements require the use of conventional adhesives or selfetching adhesive systems. The sensitivity of the technique and the difficulty of a proper sealing associated to conventional adhesives probably lead to a high incidence of postoperative sensitivity related to cementation procedures of indirect restorations 1,12,16. The self-adhesive resin cements, however, do not require pre-treatment of the tooth structure using adhesives, thereby simplifying the clinical steps during the installation of restorations procedures. For these products (pH ≈ 2.0), the smear layer is not removed and no postoperative sensitivity is expected. In addition, the pulp's inflammatory response is low and release of fluoride ions can be observed. Differently, the pretreatment of the ceramic restoration is necessary 10,13,18,19.
Guarda et al. 7 describe ceramics as materials used for dental restorations which have excellent properties, such as chemical stability, biocompatibility, low thermal conductivity, high compressive strength, translucency, fluorescence, and a coefficient of thermal expansion similar to tooth structure. To further improve these properties, many technological advances have recently enabled the development of new materials with higher mechanical strength, such as those reinforced by leucite, lithium disilicate, infiltrated by glass, injected and machined 14.
For this study, samples of ceramics reinforced by leucite strongly established in the market were used, like Creation, Finesse, IPS Empress Esthetic, and Vita PM9. They were blasted with aluminum oxide, conditioned by hydrofluoric acid followed by the application of a silane. The blasting with aluminum oxide is used to increase the surface roughness, as well as clean and activate the surface, according to several authors 5,8,14,15,17. The hydrofluoric acid works by creating pores on the surface through preferential dissolution of the glassy phase of the ceramic matrix 6,11. According to Fabianelli et al. 5, the complete removal of the restoration acid, still is necessary due to its high chemical toxicity. Some residual products of insoluble salts may remain after the conditioning of the surface. In some ceramics that are being developed, such as those based on zirconia, the crystal structure may not benefit from hydrofluoric acid. Matinlinna et al. 11 described that the role of the silane would be both physically, to increase the wettability of the ceramic surface making it more receptive to cement, as chemistry, by interaction with the cement and its inorganic particles. Indeed, it is important to remark that the adhesion of agents called silanes are synthetic hybrid components, inorganics and organics at the same time, which are used to promote adhesion between structurally different materials. Therefore, silanes are ideal to promote adhesion in restorative materials silica-based, as most of the ceramics. However, on the restorations based on zirconia and metallic alloys, the adhesion is not satisfactory, and in these cases specific primers are needed.
Taking into consideration the bond strength within each type of ceramic and one year of storage in distilled water, the means of RelyX U200 selfadhesive cement were significantly higher than that of conventional RelyX ARC for all the tested ceramics, repeating which also happened in the one-week study originally proposed in 2012 by Garcia et al. 6 (tables II and III). The resin matrix of the U200 consists of multifunctional acids and methacrylate monomers. If a large amount of these resin monomers could interact with leucite-reinforced ceramics in the proposed times and reached higher bond strength, it is possible to suggest that this resin cement can be used in reliable way 19. The findings of Özcan and Vallittu 15, however, showed a significant decrease in bond strength values for all surface treatment methods tested after thermal cycling, differently from that of this study which degraded samples in distilled water for one year. For Liu et al. 10, who conducted a similar study also using thermal cycling, the results showed that the tested self-adhesive resin cement presented sorption and solubility significantly higher than that of conventional resin cements, but the statistical analysis showed lower bond strength for all the groups.
In a qualitative analysis, Slavcheva et al. 18 evaluated the marginal adaptation and fracture strength of crowns made of ceramic reinforced with leucite (IPS Empress CAD / Ivoclar Vivadent) and cemented with a self-adhesive cement RelyX U200. Using thermal cycling as adhesive degradation method, they observed that there was no significant difference in the continuous margins that could be detected on the groups contaminated with saliva, water, blood, and control; as well as there was no difference in the marginal adaptation between the groups. Regarding the resistance to fracture, there was also no statistically significant difference between the groups. Additionally, the in vivo studies of Taschner et al. 20 with RelyX U200, which included several criteria such as surface roughness, color, anatomical shape, marginal integrity, dental health, integrity of inlay and onlay and proximal contacts, among others, ratified that this cement had acceptable behavior after two-year clinical evaluation. The authors report that the complex chemical composition of the RelyX U200 tends to have higher tolerance to humidity when compared to the more sensitive technique of conventional resin cements.
Taking into consideration the bond strength within each type of cement, the SBS means of all ceramics cemented with ARC were statistically lower after one-year storage in distilled water. By using cement U200, the same did not happen with the FIN and IEE ceramics, which presented higher SBS means and statistical differences when compared to the ceramics CRE and PM9. Guarda et al. 7 and Hopp et al. 9 reported that the clinical success and the bond strength in the ceramic restorations depend on several factors, such as the cements, the cementation procedures and the composition of the ceramics. Therefore, the group: 1) blasting with aluminum oxide that causes different patterns of roughness on the surfaces of several ceramics; 2) etching with hydrofluoric acid that can equally remove the glass matrix in a different way due to the manufacturer; 3) silanization forming a chemical interaction between the inorganic phase of the ceramic and the organic phase of the resin cement – besides the specific compositions and properties of resin cements – may be the main reason for the differences between the bond strengths. By extension, it is possible to confirm that this interaction of factors may have also contributed to the non-occurrence of the degradation (regarding to SBS) after one year of storage in distilled water in the U200 group with FIN and IEE ceramics.
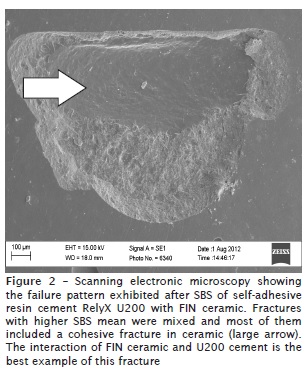
The shear bond strength tests tend to produce mixed failures, between adhesives, and cohesive in the substrate, according to many authors 4,6,17,20. Figures 1 and 2 illustrate the predominant fracture patterns for groups that resulted in lower and higher shear bond strength mean.
Conclusion
The ARC cement SBS was significantly lower for all ceramics after aging than that of U200 cement. The ARC cement (SBS) was also weakened the most by aging. FIN ceramic with U200 cement proved to be the most stable and strongest bond strength, and PM9 with ARC cement proved to be the weakest bond strength with low stability.
Acknowledgments
This study was supported by University of the Region of Joinville (Univille), Joinville, SC, Brazil (Dept of Dentistry), in partnership with Virginia Commonwealth University (VCU), Richmond, VA, USA (Dept of General Practice, School of Dentistry). Scanning Electron Microscopy was performed at the VCU (Department of Neurobiology & Anatomy Microscopy Facility), supported with funding from NIH-NINDS Center core grant 5P30NS047463 and NIH-NCRR grant 1S10RR022495.
References
1. Badini SRG, Tavares ACS, Guerra MAL, Dias NF, Vieira CD. Cimentação adesiva – revisão de literatura. Revista Odonto. 2008;32:105-15.
2. Blatz MB, Dent M, Sadan A, Kern M. Resinceramic bonding: a review of the literature. J Prosthet Dent. 2003;89(3):268-74.
3. Denry I, Holloway JA. Ceramics for dental applications: a review. Materials. 2010;3:351-68.
4. Dundar M, Ozcan M, Gokçe B, Çomlekoglu E, Leite F, Valandro LF. Comparison of two bond strength testing methodologies for bilayered allceramics. Dent Mater. 2007;23:630-36.
5. Fabianelli A, Pollington S, Papacchini F, Goracci C, Cantoro A, Ferrari M et al. The effect of different surface treatments on bond strength between leucite reinforced feldspathic ceramic and composite resin. J Dent. 2010;38:39-43.
6. Garcia RN, Nascimento RF, Gomes ACR, Giannini M, Miguel LCM, Moon PC. Bond strength of resin cements to leucite-reinforced ceramics. RSBO. 2012;9:183-89.
7. Guarda GB, Correr AB, Gonçalves LS, Costa AR, Borges GA, Sinhoreti MA et al.Effect of surface treatments, thermocycling, and cyclic loading on the bond strength of a resin cement bonded to a lithium disilicate glass ceramic. Oper Dent. 2013;38(2):208-17.
8. Hilgert LA, Junior SM, Vieira LCC, Gernet W, Edelhoff D. A escolha do agente cimentante para restaurações cerâmicas. Clínica Internacional Journal of Brazilian Dentistry. 2009;5(2):194-205.
9. Hopp CD, Land MF. Considerations for ceramic inlays in posterior teeth: a review. Clinical Cosmetic and Investigational Dentistry. 2013;5:21-32.
10. Liu Q, Meng X, Yoshida K, Luo X. Bond degradation behavior of self-adhesive cement and conventional resin cements bonded to silanized ceramic. J Prosthet. 2011;13:177-84.
11. Matinlinna JP, Lassila LVJ, Ozcan M, Urpo AY, Vallittu PK. An introduction to silanes and their clinical applications in dentistry. Int J Prosthod. 2004;17:155-64.
12. Meyer Filho A, Souza CN. Desmistificando a cimentação adesiva de restaurações cerâmicas. Clínica Internacional Journal of Brazilian Dentistry. 2005;7(1):50-7.
13. Namoratto LR, Ferreira RS, Sampaio Filho HR, Ritto FP. Cimentação em cerâmicas: evolução dos procedimentos convencionais e adesivos. Rev Bras Odontologia. 2013;70(2):142-7.
14. Neis CA, Albuquerque NL, Albuquerque Ide S, Gomes EA, Souza-Filho CB, Feitosa VP et al.Surface treatments for repair of feldspathic, leucite – and lithium disilicate – reinforced glass ceramics using composite resin. Braz Dent Journal. 2015;26(2):152-5.
15. Ozcan M, Vallittu PK. Effect of surface conditioning methods on the bond strength of luting cement to ceramics. Dent Mater. 2003;19:725-31.
16. Ribeiro CMB, Lopes MWF, Farias ABL, Cabral BLAL, Guerra CMF. Cimentação em prótese: procedimentos convencionais e adesivos. Int J Dent. 2007;6(2):58-62.
17. Shimada Y, Yamaguchi S, Tagani J. Microshear bond strength of dual-cured resin cement to glass ceramics. Dent Mater. 2002;18:380-8.
18. Slavcheva S, Krejci I, Bortolotto IT. Luting of ceramic crowns with a self-adhesive cement: effect of contamination on marginal adaptation and fracture strength. Med Oral Patol Oral Cir Bucal. 2013;18(5):799-803.
19. Souza TR, Leão Filho JCB, Beatrice LCS. Cimentos auto-adesivos: eficácias e controvérsias. Revista Dentística online. 2011;10(21):20-5.
20. Taschner M, Krämer N, Lohbauer U, Pelka M, Breschi L, Petschelt A et al. Leucite-reinforced glass ceramic inlays luted with self-adhesive resin cement: a 2-year in vivo study. Dent Mater. 2012;28:535-40.
 Corresponding author:
Corresponding author:
Rubens Nazareno Garcia
Universidade da Região de Joinville
Departamento de Odontologia
Rua Paulo Malschitzki, n.° 10
Zona Industrial – Bom Retiro
CEP 89219-710 – Joinville – SC – Brasil
E-mail: rubensngarcia@gmail.com
Received for publication: January 6, 2016
Accepted for publication: May 23, 2016
