










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRSBO (Online)
versão On-line ISSN 1984-5685
RSBO (Online) vol.13 no.3 Joinville Jul./Set. 2016
ORIGINAL RESEARCH ARTICLE
Prevalence of major apical foramen mismatching the root apex in root canals of human permanent teeth
Liana Freire de BritoI; Sylas Jamerson Sá NogueiraII; Claudio Maniglia FerreiraIII; Fabio de Almeida GomesIII; Bruno Carvalho de SousaI
I Department of Dentistry, Federal University of Ceará – Sobral – Ceará – Brazil
II Department of Dentistry, São Leopoldo Mandic School – São Paulo – Brazil
III Department of Dentistry, University of Fortaleza – Fortaleza – Ceará – Brazil
ABSTRACT
Introduction: The periapical radiograph is used to determine the working length in endodontic treatment. However, this radiograph does not define the position of the major apical foramen. Objective: This ex vivo laboratorial study aims to determine the prevalence of the major apical foramen mismatching the root apex in human permanent teeth, because when present, this mismatch makes the radiographic method inaccurate for determining the working length. Material and methods: This study used 400 human permanent teeth: 100 incisors, 100 canines, 100 premolars, and 100 molars, totalizing 634 canals (Ethics Committee, Federal University of Ceará #263/10). The access and negotiation of the root canals were performed with K-type files #10 and #15 until the tip of the instrument were visible at the root foramen through 5-fold magnifying glass. Periapical radiographs were performed on bucco-lingual incidence for single-rooted teeth; the incidence angle was changed for multi-rooted teeth. The films were processed and then analyzed by three calibrated examiners (Kappa 80%). Descriptive statistics and chi-square test were used for analyzing of the results. Results: The prevalence of major apical foramens mismatching the root apex was 19.72% of the canals studied. The incisors showed the lowest prevalence (9%, p<0.05) while the highest prevalence was seen in canine teeth (28%). Conclusion: According to the methodology applied, the prevalence of major apical foramens mismatching the root apex foramens make necessary an adjunct method for determining the working length, because it alone was not capable of determining the foramen position.
Keywords: dental pulp cavity; tooth apex; dental radiography.
Introduction
The success of endodontic treatment is closely related to the anatomical knowledge of the root canal system and its possible variations 3,18,24. This is because the proper execution of the therapy steps depends on the correct determination of the root canal apex, so that the working length is measured 5,17, allowing the cleaning, modeling, hermetic sealing, and obtaining an environment conducive to the repair of the periradicular tissues 18. Such procedures should be confined to the canal to prevent damage to periapical tissue and minimize extrusion of endodontic sealers towards the apex, which could adversely affect the success of therapy 9,19.
The apical constriction, which corresponds to the smallest diameter of the root canal has been recommended as the ideal apex limit for root canal instrumentation and filling 9-11,15,18,19. The apical constriction is at an average distance of 0,59 mm below the major foramen and 0,89 mm below the root apex 12. Because the apical constriction is a histological landmark impossible to be clinically determined, it is suggested that the major foramen should be the most reproducible position to measure the working length 7.
Historically, the periapical radiograph is the main determination method of the working length. However, this radiograph has some limitations, because it is a two-dimensional image of a tridimensional object and it not show the position of the major apical 5,14,24. By considering the distance between the apical constriction and the apical foramen, traditionally, the working length is set at 1 mm below the radiographic root apex 4,7,8. Although the major apical foramen is closely related to the root apex, they can mismatch 18,25. The center of the major apical foramen is far from the center of the root apex (anatomic or radiographic apex) in 60% to 94% of the teeth 2,6. The more recent studies show that the major apical foramen mismatched the root apex in 41.6% 24 and 49.4% 5. The working length set at 1 mm below the radiographic apex may result in over preparation and over filling, i.e., beyond the clinically acceptable limit, in cases where the major apical foramen mismatch the root apex 24.
It is mandatory to know the prevalence of this mismatch for the different tooth type and the radiographic agreement ratio between the major apical foramen and root apex because the root apex is the main landmark to determine the radiographic working length 16.
Thus, this study aimed to determine the prevalence of mismatching between the major apical foramen and the root apex in human permanent teeth, observed in radiographs.
Material and methods
This ex vivo laboratorial study was submitted and approved by the Institutional Review Board regarding the ethical aspects (protocol #263/10).
Sample selection
Four hundred human permanent teeth were studied: 100 incisors, 100 canine teeth, 100 premolars, and 100 molars, obtained in the Basic Health Units of the state of Ceara, after the signing of a Tooth Donation Form. The teeth were kept in 10% formalin then washed, and decontaminated with sodium hypochlorite for using in the study. Exclusion criteria included teeth with incomplete rhizogenesis, root apex fracture, and root resorption.
Tooth preparation
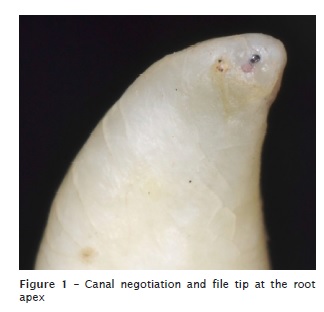
The conventional crown access was performed with round (#1012, #1014, and #1016) and flatend taper (#308) diamond burs (KG Sorensen, Barueri, São Paulo, Brasil). The root canals were negotiated with the aid of K-type files size #10 and #15 (Dentsply, Maillefer, Ballaigues, Switzerland) until the file tip was seen at the root apex with the aid of a magnifying glass at 5-fold magnification (Civiam, São Paulo, Brazil) (figure 1).
At that position, periapical radiographic were obtained with E type radiographic films (Kodak, São Paulo, Brazil), and x-ray device set at 70 Kvp and 10 mA (Dabi Atlante, São Paulo, Brazil) with exposure time of 0,2 second (figure 2).
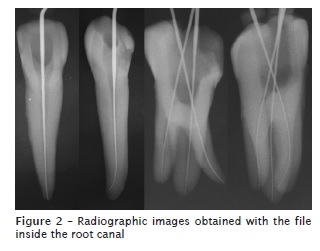
Periapical radiographs were performed on bucco-lingual incidence for single-rooted teeth. The incidence angle was changed for multi-rooted teeth. The film dot was standardized as the landmark of the mesial surface of the tooth, allowing to identify the root canals in multi-rooted teeth.
The films were developed inside a portable acrylic darkroom, through time-temperature method, dried and properly recorded according to the tooth type, and then filed. Radiographic analysis Three previously calibrated examiners (Kappa test = 80%) analyzed the radiographs by filling in a chart of the presence or absence of the mismatch between the major apical foramen and root apex. To evaluate the mismatch, a line was marked perpendicular to the canal long axis, on the apical third. The point where the line pass through the radiographic apex was considered the radiographic landmark of the root apex. The file tip was the landmark for the major apical foramen position. Statistical analysis The results obtained in the radiographic analysis was registered in percentage of prevalence. The Chi-square test was used to compare the prevalence of the mismatch among tooth types. The level of significance was set at 5%.
Results
This study found and negotiated 634 root canals in 400 teeth analyzed, comprising 100 canals for incisors, 100 canals for canine teeth, 137 canals for premolars, and 297 canals for molars. Of the 634 root canals, 125 major apical foramen mismatched the root apex, totalizing 19.72% of the cases (table I).
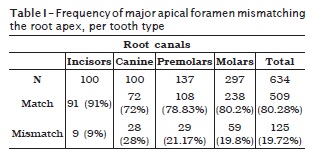
The incisors showed the smallest prevalence of the mismatch (p<0.05), followed by the canine teeth (28%), which was statistically different from the incisors (p<0.05), but without statistically difference from the premolars and molars (p>0.05). Both the incisors and canine had one root canal negotiated per tooth.
When the number of canals with mismatch was evaluated, no statistically difference occurred between premolars and molars (p>0.05). Notwithstanding, a significantly higher number of molars than premolars exhibited the mismatch (p<0.05).
Of the 297 root canals of permanent molars, 59 major apical foramens mismatched the root apex (19.8%). The mismatch occurred in 18.6% and 22.5% of the mandibular and maxillary molars.
For the different tooth types, the mismatch (n=125) occurred in 7.2% of incisors, 22.4% of canine teeth, 23.2% of premolars, and 47.2% of molars. For the whole sample (n=400), 101 teeth (25.25%) had the mismatch in at least one root canal, approximately one quarter of the sample. Of 101 teeth, the mismatch occurred in nine incisors, 28 canine teeth, 23 premolars, and 41 molars. The highest prevalence was observed in the molars, followed by the canine teeth, and premolars (table II).

Discussion
This study analyzed the prevalence of major apical foramen mismatching the root apex in 400 human permanent teeth. The results obtained revealed a total of 125 mismatches. This is 19.72% of the 634 root canals negotiated. These data showed that, in most cases, the major apical foramen matched the root apex for the different tooth types. Notwithstanding, a significant percentage of mismatch occurred. This finding shed light on the clinical practice, because the cementum canal, the apical foramen, the apical constriction, are the main landmarks to determine the apical limit of root canal preparation and filling 20.
The radiographic determination of the working threshold is based on establishing the working length, whose value is 1 mm below the radiographic root apex 16. Such measurement requires the working below the apical constriction, which is generally located from 0.5 to 0.7 mm below the apical foramen. To allow that this step-back is favorable to the endodontic preparation and filling, the major apical foramen should match the root apex. However, this fact does not occur for all cases 12. From a clinical point of view, the mismatch between the major apical foramen and the root apex put the radiographic method in question by increasing the risk of over preparation and overfilling, which may damage the apical periodontium and contribute for maintaining the chronic inflammatory process at medium and long term, even slowing the healing of the periapical tissues 7,9,16,18,19.
Salonski et al. 22 found 36% of the mismatch in 100 human permanent canine teeth. This finding is close to that obtained by this present study for the same tooth type (28%).
The distance and the location between the major apical foramen and the root apex was evaluated in 926 maxillary and mandibular teeth and the mismatch occurred in 61% of the teeth, with greater frequency for the posterior (43%) than the anterior teeth (17%) 13. This high prevalence disagrees with that found by this present study (25.25%) on 400 human permanent teeth.
Of 356 root canals studied, 176 major apical foramen mismatched the root apex 5, totalizing 50% of the teeth examined. In this present study, 101 teeth (25.25%) showed at least one major foramen mismatched from the root apex. The highest prevalence of teeth with at least one mismatch occurred for the molars, followed by the canine teeth, and premolars. Again, from a clinical point of view, this is an important finding because the presence of one mismatch may compromise the endodontic treatment success.
In the posterior teeth, the presence of more than one mismatch was common. Of 634 root canals, 125 showed the mismatch (19.72%). Awawdeh et al. 2008 1 investigated the root canal morphology of 600 maxillary premolars in Jordanians and found 40% of mismatches. In this present study, of the 100 premolars analyzed, 137 root canals showed the mismatch (21.17%).
Such findings of the high prevalence of mismatches shed light on the need of using electronic locators as adjunct tools because they allow the location of the major apical foramen even in these situations 4,5,11,23.
Notwithstanding, electronic apical locators should not replace the radiographic techniques 21. The radiographic method is still the most used and it is essential for diagnosing, determining the working length, evaluating the final endodontic filling, and following-up 24. In most of the cases, the radiographic method is accurate and reliable, but it is contraindicated in the cases whose major apical foramen mismatch the root apex 4. Because the mismatch does not have any clinical signs and in these cases the radiographic method is inaccurate, the association of the apex locator is indicated.
This study's results suggested that the periapical radiograph is a reasonable and limited method to determine the working length. The percentage of major apical foramen mismatching the root apex suggested the indication of adjunct methods that use the apical foramen as landmark.
Conclusion
According to the methodology applied and results obtained by this study, it can be concluded that the prevalence of major apical foramen mismatching the root apex was 19.72%. This finding reaffirm the limitation of the radiographic method in determining the preparation and filling length in human permanent teeth in such cases.
References
1. Awawdeh L, Abdullah H, Al-Qudah A. Root form and canal morphology of jordanian maxillary first premolars. J Endod. 2008 Aug;34(8):956-61. [ Links ]
2. Burch JG, Hulen S. The relationship of the apical foramen to the anatomic apex of the tooth root. Oral Surg Oral Med Oral Pathol. 1972 Aug;34(2):262-8.
3. Cleghorn BM, Christie WH, Dong CC. The root and root canal morphology of the human mandibular second premolar: a literature review. J Endod. 2007 Sep;33(9):1031-7.
4. D'Assunção FL, de Albuquerque DS, de Queiroz Ferreira LC. The ability of two apex locators to locate the apical foramen: an in vitro study. J Endod. 2006 Jun;32(6):560-2.
5. Ding J, Gutmann JL, Fan B, Lu Y, Chen H. Investigation of apex locators and related mo rpho l o g i c a l f a c t o r s . J Endod. 2010 Aug;36(8):1399-403.
6. Green D. Stereomicroscopic study of 700 root apices of maxillary and mandibular posterior teeth. Oral Surg Oral Med Oral Pathol. 1960 Jun;13:728-33.
7. Hassanien EE, Hashem A, Chal f in H. Histomorphometric study of the root apex of mandibular premolar teeth: an attempt to correlate working length measured with electronic and radiograph methods to various anatomic positions in the apical portion of the canal. J Endod. 2008 Apr;34(4):408-12.
8. Heidemann R, Vailati F, Teixeira SC, Oliveira CA, Pasternak Junior B. Análise comparativa ex vivo da eficiência na odontometria de três localizadores apicais eletrônicos: Root ZX, Bingo 1020 e Ipex. RSBO. 2009 Sep;6(1):7-12.
9. Herrera M, Ábalos C, Jiménez-Planas A, Llamas R. Influence of apical constriction diameter on Root ZX apex locator precision. J Endod. 2007 Aug;33(8):995-8.
10. Herrera M, Ábalos C, Lucena C, Jiménez-Planas A, Llamas, R. Critical diameter of apical foramen and of file size using the Root ZX apex locator: an in vitro study. J Endod. 2011 Sep;37(9):1306-9.
11. Jakobson SJ, Westphalen VP, Silva Neto UX, Fariniuk LF, Picoli F, Carneiro E. The accuracy in the control of the apical extent of rotary canal instrumentation using Root ZX II and ProTaper Instruments: an in vivo study. J Endod. 2008 Nov;34(11):1342-5.
12. Kuttler Y. Microscopic investigation of Root apexes. J Am Dent Assoc. 1955 May;50(5):544-52.
13. Martos J, Ferrer-Luque CM, González-Rodríguez MP, Castro LAS. Topographical evaluation of the major apical foramen in permanent human teeth. Int Endod J. 2009 Apr;42(4):329-34.
14. Martos J, Lubian C, Silveira LF, Castro LA, Luque CM. Morphologic analysis of the Root Apex in human teeth. J Endod. 2010 Apr;36(4):664-7.
15. Meder-Cowherd L, Williamson AE, Johnson WT, Vasilescu D, Walton R, Qian F. Apical morphology of the palatal roots of maxillary molars by using micro-computed tomography. J Endod. 2011 Aug;37(8):1162-5.
16. Melius B, Jiang J, Zhu Q. Measurement of the distance between the minor foramen and the anatomic apex by digital and conventional radiography. J Endod. 2002 Feb;28(2):125-6.
17. Michetti J, Maret D, Mallet JP, Diemer F. Validation of cone beam computed tomography as a tool to explore root canal anatomy. J Endod. 2010 Jul;36(7):1187-90.
18. Olson DG, Roberts S, Joyce AP, Collins DE, McPherson JC 3rd. Unevenness of the apical constriction in human maxillary central incisors. J Endod. 2008 Feb;34(2):157-9.
19. Piasecki L, Carneiro E, Fariniuk LF, Westphalen VP, Fiorentin MA, Silva Neto UX. Accuracy of Root ZX II in locating foramen in teeth with apical periodontitis: an in vivo study. J Endod. 2011 Sep;37(9):1213-6.
20. Ponce EH, Vilar Fernández JA. The cementodentino- canal junction, the apical foramen, and the apical constriction: evaluation by optical microscopy. J Endod. 2003 Mar;29(3):214-9.
21. Saghiri MA, Asgar K, Boukani KK, Lotfi M, Aghili H, Delvarani A et al. A new approach for locating the minor apical foramen using an artificial neural network. Int Endod J. 2012 Mar;45(3):257-65.
22. Salonski CC, Costa EM, Lopes HL, Deonizio MD, Westphalen VP, Silva Neto UX et al. Avaliação da posição do forame apical em caninos humanos. RSBO. 2004 Nov;1(1):14-6.
23. Tsesis I, Blazer T, Ben-Izhack G, Taschieri S, Del Fabbro M, Corbella S et al. The precision of electronic apex locators in working length determination: a systematic review and metaanalysis of the l i terature. J Endod. 2015 Nov;41(11):1818-23.
24. Vieyra JP, Acosta J. Comparison of working length determination with radiographs and four electronic apex locators. Int Endod J. 2011 Jun;44(6):510-8.
25. Villas-Bôas MH, Bernardineli N, Cavenago BC, Marciano M, Carpio-Perochena A, Moraes IG et al. Micro-computed tomography study of the internal anatomy of mesial root canals of mandibular molars. J Endod. 2011 Dec;37(12):1682-6.
 Corresponding author:
Corresponding author:
Liana Freire de Brito
Rua Coronel Estanislau Frota, n. 316
Centro
CEP 62010-560
Sobral – CE – Brasil
E-mail: lianafbrito@hotmail.com
Received for publication: July 6, 2016
Accepted for publication: August 8, 2016
