










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRSBO (Online)
versão On-line ISSN 1984-5685
RSBO (Online) vol.13 no.3 Joinville Jul./Set. 2016
CASE REPORT ARTICLE
Stabilizing periodontally compromised teeth with glass fiber-reinforced composite resin – case report
Carla Kuroki Kawamoto PereiraI; Vanara Florêncio PassosI; Sérgio Luís da Silva PereiraI
I Dentistry Course, University of Fortaleza – Fortaleza – CE – Brazil
ABSTRACT
Introduction: The tooth mobility due to periodontal bone loss can cause masticatory discomfort, mainly in protrusive movements in the region of the mandibular anterior teeth. Thus, the splinting is a viable alternative to keep them in function satisfactorily. Objective:This study aimed to demonstrate, through a clinical case with medium-term following-up, the clinical application of splinting with glass fiber-reinforced composite resin. Case report: Female patient, 73 years old, complained about masticatory discomfort related to the right mandibular lateral incisor. Clinical and radiographic evaluation showed grade 2 dental mobility, bone loss and increased periodontal ligament space. The proposed treatment was splinting with glass fiber-reinforced composite resin from the right mandibular canine to left mandibular canine. Results: Four-year follow-up showed favorable clinical and radiographic results with respect to periodontal health and maintenance of functional aspects. Conclusion: The splinting with glass fiber-reinforced composite resin is a viable technique and stable over time for the treatment of tooth mobility.
Keywords: dental occlusion traumatic; tooth mobility; polyethylene.
Introduction
The bone loss caused by periodontitis progression may lead to tooth mobility, causing discomfort during mastication, difficult in oral hygiene (because the patient fears of performing tooth brushing), perpetuating the infectious-inflammatory process and consequently evolving to tooth loss. This tooth mobility is caused by the change of the rotation fulcrum of the teeth to a more apical position 2 and may be aggravated by traumatic occlusal forces, mainly in teeth with reduced periodontium14.
In these cases, the splinting of teeth with mobility to the stable adjacent teeth is a viable alternative with clinical application in contemporary Dentistry. Splinting can be achieved with orthodontic wires associated with resin composite, orthodontic brackets and passive orthodontic wires, or resin composite alone. Until now, these aforementioned materials do not show the adequate stability and do not enable obtaining a single unit between the tooth/ splinting, which makes difficult to distribute the masticatory forces and the oral hygiene 3,14.
A very viable and promising alternative is the use of twisted polyethylene fiber ribbons bonded to the tooth surfaces 5,14. These fibers are functional, esthetic, and improve the stability of teeth with mobility due to bone loss 4,12,13.
The literature reports some cases with splinting by glass fiber-reinforced composite resin, but with short following-up periods 7,9,13. This case report aimed to describe the applicability of glass fiber-reinforced composite resin for stabilizing periodontally compromised teeth at medium-term following-up.
Case report
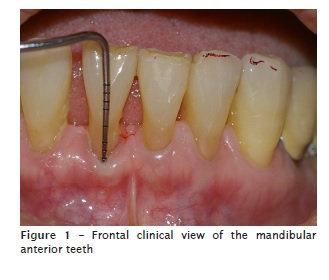
Patient MKK, female, aged 73 years, was referred to the institutional Dentistry Clinics complained about tooth mobility of the right mandibular lateral incisor and masticatory discomfort. At the intraoral examination, we noted gingival recession and loss of the interdental papilla, but without periodontal pocket (figure 1). Tooth contacts occurred on the incisal surfaces of teeth #31 and #32; teeth #41 and #42 showed weariness on the incisal surfaces (figure 1).
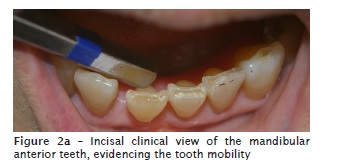
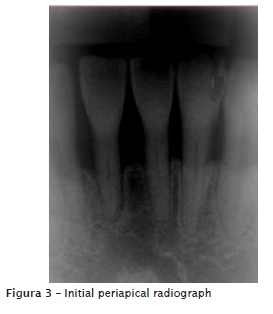
The teeth were submitted to pulp sensitivity test and showed positive results. The tooth mobility test showed degree 2 mobility in tooth #42, due to bone loss because of previously treated chronic periodontitis associated with a traumatic occlusion (figures 2 and 2a). The initial periapical radiograph diagnosed the increase in the space of the periodontal ligament, horizontal bone loos compromising half of the root surface, and bone resorption on the alveolar ridge (figure 3).

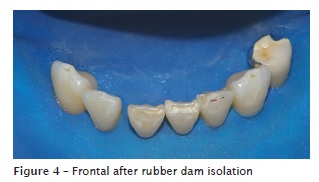
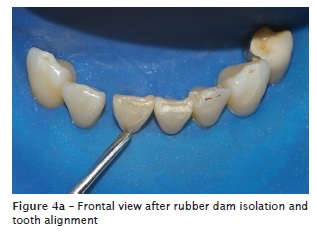
The proposed treatment was splinting the teeth #43 to #33 with resin composite reinforced by twisted glass fiber. After rubber dam isolation, tooth #42 was placed into position and aligned with the other anterior teeth (figures 4 and 4a).
After tooth prophylaxis with pumice and Robson brush (Microdont) at low speed, the enamel surfaces were conditioned with 37% phosphoric acid (FGM) for 30 seconds and washed for 30 seconds, dried, and followed by the application of the adhesive agent (Scotchbond-3M ESPE).
The glass fiber (Interlig, Ângelus) was cut and adapted onto the lingual surfaces, according to the manufacturer's instructions (figure 5). Then, all ribbon was covered by resin composite (Filtek Z250 XT, 3M ESPE). This same material was used to obtain the proximal contact point between teeth #42 and #43 and partially reconstruct the incisal surfaces (figure 6). The patient was instructed to performed oral hygiene with interdental toothbrushing, changed at every three months. After one week, the finishing and polishing procedures were carried out with sandpaper disc (Sof-lex, 3M) and felt discs with polishing paste (Poli Composta, Asfer).


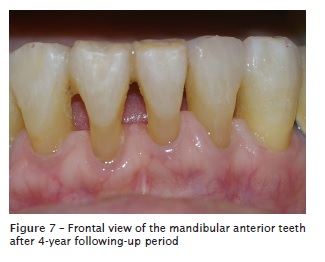
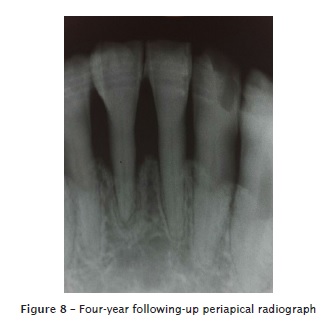
After four years, we observed the periodontal health and the complete and functional splinting, maintaining the masticatory comfort (figure 7). Radiographically, no further periodontal insertion loss was noted, but the reduction of the periodontal ligament space and bone deposition on the apical, lateral and alveolar ridge areas (figure 8).
Discussion
The tooth degree is directly related to the amount of remaining bone and root length and shape 2,14. Single-rooted teeth have more pronounced mobility than do multi-rooted teeth, mainly when the loss of alveolar insertion reaches half of the root 2,14.
Teeth with mobility were not more susceptible to greater insertion loss over time 6, but these teeth may cause masticatory discomfort, as reported in this clinical case. Thus, the splinting restores the functional occlusion and the masticatory comfort, improves the esthetics, and promotes the psychologic well-being of the patient 12.
Tooth mobility itself is not indicative of tooth splinting, but occlusal adjustment associated to splinting may avoid the progressive loss of tooth insertion 4, because this procedure adjusts the rotation fulcrum of the teeth with mobility on the bone remnant preventing the load excess of masticatory forces22.
Although the effectiveness of the materials for splinting seems indifferent, the twisted glass fiber has some advantages over the stainless steel wire and resin composite 1,11,17. Bond strength tests of specimens made of glass-fiber reinforced resin composite showed the increasing of the bond strength and the modulus of elasticity compared with the specimens made of resin composite alone5,21.
The glass fiber shows long-term success rate due to the esthetic features of the resin composite associated with the strength of the thin ribbon treated by plasma with chemical and adhesive reinforcement with high modulus of elasticity and effective resistance to the occlusion and masticatory forces20. These characteristics are evidenced by this case report.
It is worth noting that splinting makes oral hygiene difficult and special attention is needed to assure long-term success of splinted teeth 15. In this case report, we avoid to close the diastemas between the incisors which allowed an easier oral hygiene with interdental toothbrushing, because that was a non-esthetic area.
The controlling of the interproximal biofilm is necessary to avoid periodontal disease10. The conventional toothbrushing reduces the supragingival biofilm in up to 40%, but it is less effective in the interproximal area 19. The interdental toothbrushing is as effective as dental floss in removing supragingival biofilm in patients requiring periodontal following-up 10.
Moreover, the interdental toothbrushing is more practical than tooth floss in cases of tooth splinting. The systematic reviews demonstrate that the association of interdental toothbrushing and conventional toothbrushing are more effective in removing biofilm and reducing gingival inflammation than conventional toothbrushing alone or associated with flossing 8,16,18.
The splinting of mandibular anterior teeth is a fast, low-cost, conservative procedure 5, with short-term successful outcomes 7,9,13. Notwithstanding, the literature lacks case reports with longer following-up periods 12. In this context, the present case report demonstrated medium-term successful outcomes.
Conclusion
Taking into consideration the function devolution, health periodontium, the 4-year following-up period, patient's level of satisfaction, and the obtained clinical success, the splinting with glass fiber reinforced resin composite is a reliable technique with excellent clinical and functional outcomes, when the patient is carefully instructed on oral hygiene.
References
1. Agrawal AA, Chitko SS. The use of silane-coated industrial glass fibers in splinting periodontally mobile teeth. Indian J Dent Res. 2011. Jul- Aug;22(4):594-6. [ Links ]
2. Alves RV, Neves RV, Lopes MWF, Gusmão ES. Mobilidade dentária: incidência, influência na terapia e relação com outras condições clínicas. Estudo retrospectivo. R PerioNews. 2009 Mar;3(3):199-203.
3. Anagnostou M, Papazoglou E, Mountouris G, Gaintantzopoulou M. Light protection of fiberreinforced strip using aluminum foil for the direct splinting technique. Oper Dent. 2006 May-Jun; 31(3):394-7.
4. Bernal G, Carvajal JC, Muñoz-Viveros CA. A review of the clinical management of mobile teeth. J Contemp Dent Pract. 2002 Nov;3(4):10-22.
5. Delfino CS, Nagle MM, Soares A, Domaneschi C. Sistemas de fibras em Odontologia. RGO. 2002 Nov-Dec; 51(5):395-400.
6. Donos N, Laurell L, Mardas N. Hierarchical decisions on teeth vs. Implants in the periodontitissusceptible patient: the modern dilema. Periodontol 2000. 2012 Jun; 59(1):89-110.
7. Friskopp J, Blomlof L. Int e rmedi a t e fiberglass splints. J Prosthet Dent. 1984 Mar; 51(3):334-7.
8. Gluch JI. As an adjunct to tooth brushing, interdental brushes (IDBs) are more effective in removing plaque as compared with brushing alone or the combination use of tooth brushing and dental floss. J Evid Based Dent Pract. 2012 Jun; 12(2):81-3.
9. Heinz B. Fabrication and strategic significance of a special resin composite splint in advanced periodontitis . QuintessenceInt . 1996 Jan;27(1):41-51.
10. Jordan RA, Hong HM, Lucaciu A, Zimmer S. Efficacy of straight versus angled interdental brushes on interproximal tooth cleaning: a randomized controlled trial. Int J Dent Hyg. 2014 May;12(2):152-7.
11. Khetarpal A, Talwar S, Verma M. Single visit rehabilitation with anterior fiber reinforced resin composite bridges: a review. Indian J Appl Res. 2013 Feb;3(2):287-9.
12. Kumbuloglu O, Aksoy G, User A. Rehabilitation of advanced periodontal problems by using a combination of a glass fiber-reinforced composite resin bridge and splint. J Adhes Dent. 2008 Feb; 10(1):67-70.
13. Meiers JC, Duncan JP, Freilich MA, Goldberg AJ. Preimpregnated, fiber-reinforced prostheses. PartII. Direct applications: splints and fixed partial dentures. Quintessence Int. 1998 Dec;29(12):761-8.
14. Newman MG, Takei H, Klokkevold PR, Carranza FA. Periodontia Clínica. 11. ed. São Paulo: Elsevier; 2012. p. 812-4.
15. Puri MS, Grover HS, Gupta A, Puri N, Luthra S. Splinting – A healing touch for an ailing periodontium. J Oral Health Comm Dent. 2012 Sep;6(3):145-8.
16. Rasines G. The use of interdental brushes along with toothbrushing removes most plaque. Evid Based Dent. 2009 Jun;10(3): 74.
17. Sekhar LC, Koganti VP, Shankar BR, Gopinath A.A comparative study of temporary splints: bonded polyethylene fiber reinforcement ribbon and stainless steel wire + composite resin splint in the treatment of chronic periodontitis. J Contemp Dent Pract. 2011 Sep;12(5):343-9.
18. Slot DE, Dorfer CE, van der Weijden GA. The efficacy of interdental brushes on plaque and parameters of periodontal inflammation: a systematic review. Int J Dent Hyg. 2008 Nov;6(4): 253-64.
19. Slot DE, Wiggelinkhuizen L, Rosema NA, van der Weijden GA. The efficacy of manual toothbrushes following a brushing exercise: a systematic review. Int J Dent Hyg. 2012 Aug;10(3):187-97.
20. Strassler HE, Tomona N, Spitznagel JK. Stabilizing periodontally compromised teeth with fiber-reinforced composite resin. Dent Today. 2003 Sep;22(9):102-4.
21. Vallitu PK. Some aspects of the tensile strength of undirectional glass fibre-polymethyl methacrylate composite used in dentures. J Oral Rehabil. 1998;25(2):100-5.
22. Zarow M, Paisley CS, Krupinski J, Brunton PA. Fiber-reinforced composite fixed dental prostheses: two clinical reports. Quintessence Int. 2010;41(5):471-7.
 Corresponding author:
Corresponding author:
Sérgio Luís da Silva Pereira
Av. Engenheiro Leal Lima Verde, n. 2.086
José de Alencar
CEP 60830-055
Fortaleza – CE – Brasil
E-mail: luiss@unifor.br
Received for publication: May 6, 2016
Accepted for publication: June 8, 2016
