










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRSBO (Online)
versão On-line ISSN 1984-5685
RSBO (Online) vol.13 no.4 Joinville Out./Dez. 2016
ORIGINAL RESEARCH ARTICLE
Association of early life health conditions, nutritional status, and feeding practices with caries prevalence in preschool children
Caroline HarmatiukI; Marjorye Maceno de LimaI; Yasmine Mendes PupoII; Juliana SchaiaIII; Ana Cláudia ChibinskiIV; Marcia Helena Baldani PintoIV
I DDS – Ponta Grossa – PR – Brazil
II Departament of Dentistry, Federal University of Paraná – Curitiba – PR – Brazil
III Departament of Dentistry, Catholic University of Paraná – Curitiba – PR – Brazil
IV School of Dentistry, State University of Ponta Grossa – Ponta Grossa – PR – Brazil
ABSTRACT
Objective: This study aimed to determine whether health conditions in the first year of life, nutritional status and dietary habits throughout life are related to the prevalence of early childhood caries (ECC). Material and methods: Sample consisted of 338 children from public schools. The prevalence of dental caries was assessed by dmf-t index. An anthropometric analysis was conducted for identification of nutritional risk. Data were analyzed using Chi-square and Poisson regression analysis, considering the dependent variables: a) presence of ECC (dmft ≥ 1); b) presence of severe ECC (dmft ≥ 6). Results: It was observed that 64% of the children exhibited ECC (mean dmft 2.97) and 23% suffer from severe ECC (mean dmft 8.2). 28 (11%) were at nutritional risk and more than 30% consumed sweets one or more times a day. It was observed that 8% showed low birth weight, 9% used antibiotics frequently in the first year of life and 67% maintained the habit of nocturnal bottle/breast-feeding after this period. Nocturnal feeding for prolonged time, frequent use of antibiotics and nutritional risk were associated with higher prevalence and severity of caries in the multivariate analysis. Conclusion: These results reinforce the relationship between early life events, nutritional status, and dental caries in primary teeth.
Keywords: health care; child health; nutrition status; dental caries.
Introduction
The influence of early-life events in determining inequalities in health throughout life is well known 19. The association between accumulated social and biological risks and the occurrence of oral diseases has been the subject of research 12,22. Therefore, it has been identified the influence of the phenomena that occur in the perinatal period or in early childhood in determining dental caries many years later, such as low birthweight, some diseases or deficit in the height-to-age relationship in the first year of life, which is a synthetic indicator of nutritional status 19,23.
There is a consensus that diet and nutritional status may impact oral conditions of the children 15. Some nutrients are directly associated with tooth development and eruption and, clinically, it has been observed that individuals who experienced severe nutritional deficiencies in childhood tend to show alterations in structure and form of the enamel 31.
Nutritional status is a reliable marker of stressful early-life events 23. Malnutrition, as measured by stunting, is one of the most common nutritional deficiencies and can be caused both by inadequate food intake or recurrent infections 10. To date, studies suggest that malnutrition episodes may increase susceptibility to caries due to defects in enamel development (hypoplasia) or alterations in the salivary glands 10. Hypoplastic enamel is associated with the occurrence of early childhood caries9. In addition, malnourished children have lower buffering capacity and secretion rates of saliva, lower secretion rates of calcium and protein, and compromised immunological factors when compared to well-nourished children 19. In a four years cohort study, involving 209 Peruvian children, Alvarez 3 found that episodes of malnutrition occurring in the first year of life were associated to high incidence of caries in primary and permanent teeth.
Inadequate dietary patterns in the first years of life are usually accompanied by high consumption of sucrose. There is a positive association between sucrose intake and caries experience 22, especially if it occurs between meals or during sleep, when the protective effect of saliva is reduced due to decreased salivary flow. Children with high intake of sucrose, both in quantity and frequency, tend to show higher number of cariogenic bacteria and higher risk of developing caries, especially when they do not receive regular exposure to fluoride 12. The proposed risk models for early childhood caries showed that the contributing factors are some common variables involved in nutrition habits such as bottle-feeding, prolonged night-time breast-feeding and the consumption of sweet drinks 30.
Some studies on the relationship between early-life markers of development and dental caries indicated significant associations 19,23. Low birth weight may affect the development of tooth enamel 24. In addition to more susceptible enamel due to hypoplasia, it has been shown that low birth weight children could have lower immune function, which should favor the colonization by cariogenic microorganisms 6. One must also consider the dietary pattern resulting from this condition. Analyzing the effects of diet, breastfeeding and weaning, there are evidences showing that preterm and low birth weight infants had a higher intake of sucrose, compared to a group of full-term ones 11.
Nutritional problems are more common and severe during pregnancy (as manifested through low birth weight) and during the first year of life, both before and after weaning. They play an especially critical role in the development of deciduous dentition, due to the short period of mineralization of the teeth, when compared to the permanent dentition 17. Thus, one should expect that the susceptibility of deciduous teeth to caries is dependent on the child's nutritional history17. Moreover, poor dietary habits are more common in the early years of life, especially in low-income populations, which would increase the risk of developing severe caries 20. Based on this information, this study aims to determine whether perinatal events and health conditions in the first year of life, as well as nutritional status and dietary habits throughout life are related to the prevalence of caries in primary teeth.
Material and methods
This cross-sectional study is part of a broad research aimed to identify factors related to the presence of developmental defects of enamel and dental caries in school and preschool children. It was approved by the Ethics Committee of the State University of Ponta Grossa and by the City Department of Education. Study participants were children between 5 and 6 years old, enrolled in the first year of elementary level in public schools of Ponta Grossa (PR), whose parents signed the consent form, and who agreed to be examined.
The sample size calculation considered the population of 5 and 6 years living in the city in 2007 (11,681 children); expected prevalence of caries estimated in 50%; 5% accuracy and confidence interval of 95%, resulting in a total of 370 children. To select the sample, we included all urban schools which did not delivery school dental care (72 out of 78). Of these, 10 schools were drawn up in five different regions of the city. From this process, we selected approximately the double of the number of children necessary for research. We chose this procedure after performing a pilot study and estimating the proportion of nonparticipation. Six schools had dental offices, with dentists who provide dental care for schoolchildren. They were excluded to enable the diagnosis of the greatest possible number of untreated teeth with developmental defects of enamel.
Data collection took place through a pretested questionnaire sent to parents, as well as through oral examinations performed by four previously trained examiners. To calculate the agreement rates, we proceeded calibration exercises in which 10 children were examined by all the researchers, and re-examined after a two-day interval. The percentage of agreement were 95% or more. The lowest Kappa obtained for enamel defects and caries were respectively 0.7 and 0.8, both to the intra and inter examiner agreement.
The variables selected for this study were:
a) Dental caries – dmft index, and clinical examinations were performed according to WHO methodology, in a room with ambient light, using spatula or a tongue depressor (12). Before the clinical examination, the children brushed their teeth with a fluoridated toothpaste;
b) Perinatal conditions – birth weight data were obtained through a questionnaire answered by mothers with the help of the children's record of health history (Child Care Card from Brazilian Ministry of Health). The cutoff point was <2.500 gr., which was defined as low weight at birth according to the manual Surveillance System Food and Nutrition (SISVAN) Health Ministry 4;
c) Condition of health in the first year of life – frequency of use of antibiotics, which was reported by the mother;
d) Duration of breastfeeding and breastfeeding at night, in months, indicated by mothers in the questionnaire;
e) Nutritional risk – observed in anthropometric analysis. It was recorded age, weight and height during the examination. We used a mechanical scale, that was set to zero before each child is weighed, and stadiometer. The tests were standardized according to a previously tested methodology 16. For this study, children were classified by the parameter weight for age (WAZ) in: normal weight, nutritional risk and at risk of overweight. This is one of the indexes recommended by WHO to assess the nutritional status of children. We used the cutoffs recommended by SISVAN: ≥ 3 percentile and <10th percentile growth curve = nutritional risk, ≥ 10th percentile and <97th percentile = healthy weight or appropriate; ≥ 97th percentile growth curve = risk of overweight 4;
f) Frequency of consumption of foods containing sucrose: it was obtained using a Food Frequency Questionnaire for Children (QFAC), adapted from the category 'sugar, sweets and snacks' of the instrument developed by Colucci et al.. 8. This instrument adopts the recall period of six months preceding the application, allowing a comprehensive assessment of diet, considering the variability in children's food preferences. For each food, simple questions were established with multiple closed answers 8. We defined six categories that have been assigned scores: never (score 0), less than 1 time per week (score 1), 1 time per week (score 2), 3-4 times per week (score 3), 1-2 times a day (score 4), 3 times a day (score 5), 4 times a day or more (score 6). Responses categorized scores with 5:06 characterized frequent consumption of food.
To control the possible confounding factors, frequency of toothbrushing and the presence of developmental defects of enamel (DDE) were included in the analysis. The latter was obtained by the modified DDE index, using methods recommended by the World Health Organization (WHO).
For data analysis, we used SPSS 15.0 software for Windows. Associations were examined by chisquare test, considering two dependent variables, according to the parameters suggested by Drury et al.. 16 for studies of caries in preschool children: a) presence of early childhood caries (dmft ≥ 1) and b) presence of severe early childhood caries (dmft ≥ 6). Multivariate logistic regression analysis is the best explanatory models for caries experience in primary teeth. For this step, we selected only variables that were associated with statistical significance less than or equal to 20%.
Results
The final sample consisted of 338 children (50.2% girls and 49.7% boys) aged 5-6 years, who were present in the classrooms in the days of data collection. The sample characteristics are presented in table I. It is found that 8.0% of children born underweight and 11.2% at nutritional risk, below the appropriate weight for their age. Mothers reported that 27.6% of the children had health problems in the first year of life (data not provided in the table) and 8.8% frequently used antibiotics in this period.
Also in table I, it is observed that 39.7% of children continued to receive breast milk after 12 mont hs of life, a nd about 67% remained with breastfeeding at night after that period. High number of children used or had used the bottle (76.0%), 93 children (30.4%) used a bottle until age 4 or older, and 47 children (15.4%) still used at t he t ime of t he st udy. It was also observed that 66.6% maintained the habit of nocturnal breastfeeding after 12 months of life.
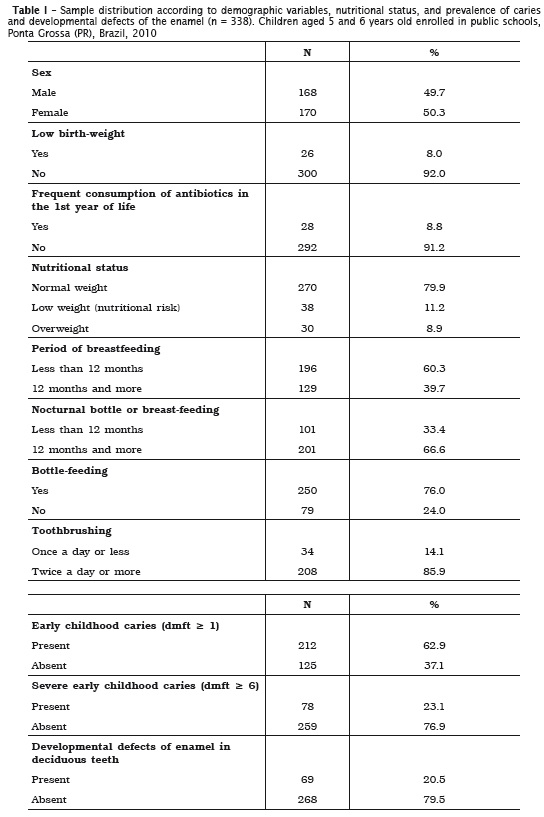
The proportion of early childhood caries was 62.9%, with a mean dmft of 2.97 (± 3.35). It was diagnosed severe caries in 23.1% of children. In this group, the mean dmft was 8.23. The mothers or caregivers informed that most of the children performed oral hygiene (98.9%) and 86% brush their teeth twice a day or more (data not included in the table).
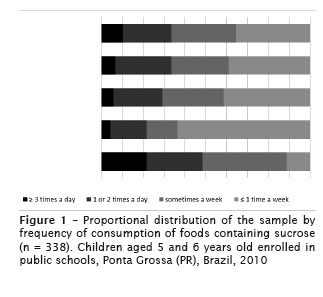
Figure 1 summarizes the information about the frequency of the consumption of sucrose. For all food groups, there was a high frequency, highlighting the fact that over 30% of children ate sweets and biscuits once a day or more. As for sweets, 10.3% of the sample reported to eat them with frequency equal to or greater than three times a day. High consumption of sweetened liquid was also observed, with 21.6% of children having them three times a day or more.
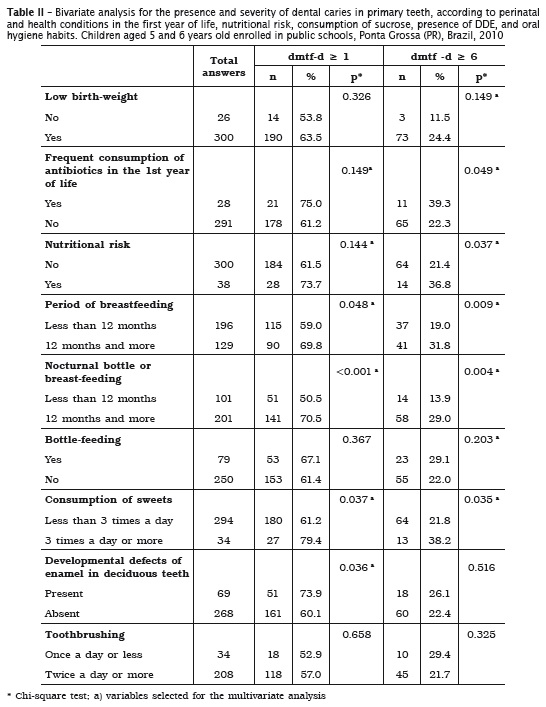
Factors related to caries experience in deciduous teeth are presented in table II.
There were no significant differences regarding gender, both for caries prevalence and for the presence of severe caries. There was greater prevalence of dental caries, considering the presence of at least one tooth affected, among chi ldren who had been breast fed or were breast fed at night after 12 months of age who consume sweets frequently less than three times a day, and having a lack of dental enamel. When the focus of analysis was the highest severity of caries experience (dmft teeth children 6 or older), it was observed that in addition to factors related to breastfeeding and diet, also showed higher prevalence among chi ldren at nutrit ional risk and those with history of frequent consumption of antibiotics in the first year of life (table II).
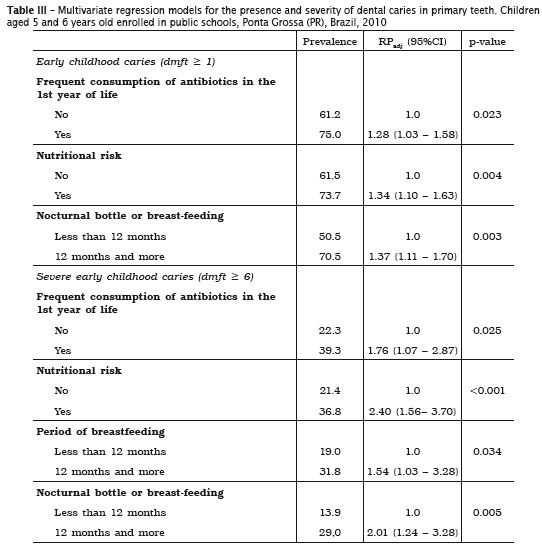
In table III there are models that explain the presence and severity of caries in deciduous teeth, obtained by multivariate Poisson regression analysis. The explanatory model for the presence of early childhood caries (in at least one tooth) includes frequent consumption of antibiotics during the first year of life, current nutritional risk and the habit of breast or bottle-feeding at night until more than the first year of life. When we consider the presence of severe caries, the explanatory model included, along with those variables included in the other model, the persistence of breast-feeding after the age one.
Discussion
Despite the decline in recent decades, dental caries is still seen as the main oral health problem in most countries, especially among children and adolescents with low incomes 7. The presence of caries carries risks to child health, and the knowledge of the determinants have been shown to be necessary to evaluate and guide practice during the prenatal and infant health, as well as interventions based on health promotion 28.
This study was conducted with a sample of children from public schools. Among them, 62.9% exhibited carious lesions in primary teeth (dmft 2.97). These results are similar to those obtained in Medellin – Colombia (54.7%; dmf-t=2.2) 26 and to the results obtained in Recife (PE) (60.6%; dmft= 2.85) 18. As in the present research, those studies found that most of teeth with carious lesions were not restored. Severe caries situation was found in 23.1% of children from our sample. These values are similar to those found in Recife (PE) (25% of children with dmft greater than or equal to 5) 18. Dental caries early established in childhood interferes in the quality of life of children and their families 25.
Adverse socioeconomic conditions during childhood are associated with poorer health and nutrition profiles. As the cavity, these are described as the result of the standard of living, which includes social and economic difficulties that are reflected in inadequate housing, undertake the acquisition of a balanced diet and difficult access to health services 27. In this sample, 11.2% of the children was at nutritional risk. In a population with good health and nutrition, it is expected that 2.3% of individuals have low or very low weight, 13.6% are at nutritional risk and 84.1% are eutrophic 29. The results of this study are consistent with these parameters.
In this study, we found an association between nutritional risk and the presence of caries, with greater strength in the case of severe caries. Similar findings were observed in Vietnam 13 and China 32. In Brazil, Oliveira et al.. 21 performed a crosssectional study involving children between 12 and 59 months of Diadema (SP) and they identified the presence of early childhood caries (dmft ≥ 1) and severe early childhood caries (dmft ≥ 6). In both cases, there was an association between caries and the mother's educational level, nutritional status, child age, and presence of clinically visible plaque. The same associations were identified by others researches in different countries 12,14.
Despite the results corroborate those described by other authors, the relationship between caries and nutritional risk is unclear, and some studies have not demonstrated this association 5. The relationship between nutritional status and caries represents a confounding factor, since the presence of severe childhood caries may affect a child's growth adversely 21, with a negative impact on the quality of life of the preschool children 27. Moreover, environmental and socioeconomic factors such as lifestyle, family, educational level and income also explain the variations in oral health status. These variables could explain the fact that the relationship between caries and nutritional risk have been shown as a non-consensus subject in the literature 15.
Several studies support the hypothesis that the relationship between nutrition and dental caries is mediated by changes in dental enamel 10,31. This study identified a positive association between developmental defects of enamel and dental childhood caries; however, this was not sustained by the multivariate analysis.
Habits in children's diet is an important factor in the etiology and progression of caries. Several studies have demonstrated the correlation between the frequency of sucrose intake at early ages and the prevalence of caries 12,22. The influence of dietary habits has been particularly evident in the case of severe early childhood caries. Habits such as unlimited use of bottle feeding, breastfeeding at night as well as the habit of breastfeeding past the age of 2 years 30 are associated with the development of early childhood caries in preschool children. Breastfeeding at night presented itself as an important determinant of caries in this study and the continuity of the habit after 12 months of life increased the odds for the presence of carious lesions as well as the possibility of increased severity. Although not included in the multivariate models, the reported frequent intake of sweets in a daily basis was also associated with higher prevalence and severity of caries in primary teeth. These results are similar to those obtained in a research involving children 6 years old in the city of Pelotas (RS) 23.
In the final model for the presence of caries severity, the factor "frequent use of antibiotics" were included. This was used as an indicator of the occurrence of recurrent infections in the first year of life. Although there is no consensus on the topic, some studies have indicated that the occurrence of frequent episodes of otitis media or respiratory tract infections and antibiotic use in the first year of life were associated with a significantly increased risk of developing early onset of decay in subsequent years 1,2. One possible explanation is the presence of sucrose and low pH of most drugs. However, one must consider that the child affected by a disease lives an extraordinary situation in which the cariogenic factors relating to food and lack of proper hygiene may prevail.
Despite having information consistent with the literature, this study has some limitations. The response rate to the questionnaires was high (58.3%), which was expected since they were sent to the parents to answer at home by the children. Thus, one should be cautious in extrapolating the results to the entire population of 5 and 6 years old in the city. Moreover, because of the crossover design of the study, the results allowed us to confirm the hypotheses regarding the factors associated with, but they have no power of causal inference.
Another limitation is related to the possibility of response bias, which affects any study based on questionnaires. Many respondents did not know properly about the frequency of children's toothbrushing. The questionnaires were completed by the mothers and the answers were dependent on the observation, which cannot be fully trusted. For example, some mothers of children presenting severe caries may have omitted data about the diet, so they would not appear negligent in the caregiving of their child. Some of the mothers interviewed may also have memory difficulties to answer the questions.
Taking all data together, it was possible to conclude that there were associations between events that occurred early in life, like feeding habits and use of antibiotics, and childhood caries. Nutritional risk, another indicator of changes in dietary patterns throughout life, was associated with greater prevalence and severity of dental caries in the studied group.
References
1. Alaki SM, Burt BA, Garetz SL. Middle ear and respiratory infections in early childhood and their association with early childhood caries. Pediatr Dent. 2008;30(2):105-10. [ Links ]
2. Alaki SM, Burt BA, Garetz SL. The association between antibiotics usage in early childhood and early childhood caries. Pediatr Dent. 2009;31(1): 31-7.
3. Alvarez JO. Nutrition, tooth development, and dental caries. Am J Clin Nutr. 1995;61(2):410S-6S.
4. Brasil. SISVAN – Orientações básicas para a coleta, processamento, análise de dados e informação em serviços de saúde. Brasília: Ministério da Saúde; 2004.
5. Brehsan TR, Vieira ARR, Peres KG. Estado nutricional na primeira infância e cárie dentária na dentição decídua: uma revisão de literatura. Rev Odontol UNESP. 2009;38(4):249-55.
6. Burt BA, Pai S. Sugar consumption and caries risk: a systematic review. Journal of Dental Education. 2001;65(10):1017-23.
7. Capurro DA, Iafolla T, Kingman A, Chattopadhyay A, Garcia I. Trends in income-related inequality in untreated caries among children in the United States: findings from NHANES I, NHANES III, and NHANES 1999-2004. Community Dent Oral Epidemiol. 2015;43(6):500-10.
8. Colucci ACA, Philippi ST, Slater B. Desenvolvimento de um questionário de freqüência alimentar para avaliação do consumo alimentar de crianças de 2 a 5 anos de idade. Rev Bras Epidemiol. 2004;7(4):393-401.
9. Corrêa-Faria P, Paixão-Gonçalves S, Paiva SM, Pordeus IA, Marques LS, Ramos-Jorge ML. Association between developmental defects of enamel and early childhood caries: a cross-sectional study. Int J Paediatr Dent. 2015;25(2):103-9.
10. Costa DP, Mota ACM, Bruno GB, Almeida MEL, Fonteles CSR. Desnutrição energético-protéica e cárie dentária na primeira infância. Rev Nutr. 2010;23(1):119-26.
11. Davenport E, Litenas C, Barbayiannis P, Williams C. The effects of diet, breast-feeding and weaning on caries risk for pre-term and low birth weight children. Int J Paediatr Dent. 2004;14(4):251-9.
12. Jain M, Namdev R, Bodh M, Dutta S, Singhal P, Kumar A. Social and behavioral determinants for early childhood caries among preschool children in India. J Dent Res Dent Clin Dent Prospects. 2015;9(2):115.
13. Khanh LN, Ivey SL, Sokal-Gutierrez K, Barkan H, Ngo KM, Hoang HT et al.. Early childhood caries, mouth pain, and nutritional threats in Vietnam. Am J Public Health. 2015;105(12):2510-7.
14. Kuriakose S, Prasannan M, Remya K, Kurian J, Sreejith K. Prevalence of early childhood caries among preschool children in Trivandrum and its association with various risk factors. Contemp Clin Dent. 2015;6(1):69.
15. Li L-W, Wong HM, Peng S-M, McGrath CP. Anthropometric measurements and dental caries in children: a systematic review of longitudinal studies. Adv Nutr. 2015;6(1):52-63.
16 . LohmanTG,RocheAF ,Martorell R . Anthropometric standardization reference manual. Human Kinetics Books; 1988.
17. Melo JAS, Couto GBL, Vasconcelos MMVB, Botelho KVG. Prevalência de hipoplasia de esmalte na dentição decídua e sua relação com o peso ao nascer. Odontol Clín-Ciênt. 2002;1(3):181-5.
18. Melo MMDC, Souza WV, Carvalho MLL, Couto GBL, Malheiros T, Paixão A. Polarização da cárie dentária em pré-escolares cadastrados no Programa Saúde da Família do Recife. Odontol Clín-Ciênt. 2009;8(1):35-40.
19. Nicolau B, Thomson W, Steele J, Allison P. Life-course epidemiology: concepts and theoretical models and its relevance to chronic oral conditions. Community Dent Oral Epidemiol. 2007;35(4):241-9.
20. Oliveira A, Chaves A, Rosenblatt A. The influence of enamel defects on the development of early childhood caries in a population with low socioeconomic status: a longitudinal study. Caries Res. 2006;40(4):296-302.
21. Oliveira LB, Sheiham A, Bönecker M. Exploring the association of dental caries with social factors and nutritional status in Brazilian preschool children. Eur J Oral Sci. 2008;116(1):37-43.
22. Peltzer K, Mongkolchati A. Severe early childhood caries and social determinants in threeyear- old children from Northern Thailand: a birth cohort study. BMC Oral Health. 2015;15(1):1.
23. Peres MA, Latorre MRD, Sheiham A, Peres KG, Barros FC, Hernandez PG et al.. Social and biological early life influences on severity of dental caries in children aged 6 years. Community Dent Oral Epidemiol. 2005;33(1):53-63.
24. Prokocimer T, Amir E, Blumer S, Peretz B. Birth-weight, pregnancy term, pre-natal and natal complications related to child's dental anomalies. J Clin Pediatr Dent. 2015;39(4):371-6.
25. Queiroz BM, de Alencar NA, Requejo MEP, Antonio AG, Maia LC. Risk factors, perception of caregivers and impact of early childhood caries on quality of life related to oral health of preschool children and their families. Brazilian Research in Pediatric Dentistry and Integrated Clinic. 2015;15(1):85-94.
26. Ramírez-Puerta BS, Franco-Cortés AM, Ochoa- Acosta E, Escobar-Paucar G. Caries experience in primary dentition in children at 5-year-old, Medellin, Colombia. Rev Facultad Nac Salud Pública. 2015;33(3):345-52.
27. Ramos-Jorge J, Ramos-Jorge ML, de Paiva SM, Marques LS, Pordeus IA. Dental caries and quality of life among preschool children. In: Virdi MS (ed.). Emerging trends in oral health sciences and dentistry. 2015.
28. Sheiham A, Conway D, Chestnutt I. Impact of oral diseases and oral health inequalities. In: Watt RG, Listl S, Peres M, Heilmann A (eds.). Social inequalities in oral health: from evidence to action. London: UCL; 2015.
29. Silva MV, Ometto AMH, Furtuoso MCO, Pipitione MAP, Sturion GL. Acesso à creche e estado nutricional das crianças brasileiras: diferenças regionais, por faixa etária e classes de renda. Rev Nutr. 2000;13(3):193-9.
30. Turton B, Durward C, Manton D, Bach K, Yos C. Socio-behavioural risk factors for early childhood caries (ECC) in Cambodian preschool children: a pilot study. Eur Arch Paediatr Dent. 2015:1-9.
31. Yadav PK, Saha S, Jagannath G, Singh S. Prevalence and association of developmental defects of enamel with, dental-caries and nutritional status in pre-school children, Lucknow. J Clin Diagn Res. 2015;9(10):ZC71.
32. Yang F, Zhang Y, Yuan X, Yu J, Chen S, Chen Z et al.. Caries experience and its association with weight status among 8-year-old children in Qingdao, China. J Int Soc Prev Community Dent. 2015;5(1):52.
 Corresponding author:
Corresponding author:
Ana Cláudia Rodrigues Chibinski
Universidade Estadual de Ponta Grossa
Faculdade de Odontologia
Av. General Carlos Cavalcanti, n. 4.748
CEP 84030-900 – Ponta Grossa – PR – Brazil
E-mail: anachibinski@hotmail.com
Received for publication: August 18, 2016
Accepted for publication: September 22, 2016
