










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRSBO (Online)
versão On-line ISSN 1984-5685
RSBO (Online) vol.13 no.4 Joinville Out./Dez. 2016
ORIGINAL RESEARCH ARTICLE
Oral health self-perception among adults at a primary healthcare unit
Nicole Paiva VerasI; Anna Claudia Dias-PereiraI; Meire Coelho FerreiraI
I Department of Dentistry, Ceuma University – São Luís – MA – Brazil
ABSTRACT
Introduction: Oral health self-perception is the individual assessment of the oral conditions. Objective: To evaluate the oral health selfperception of adults and the factors that influence this perception. Material and methods: A cross-sectional study was conducted at a primary healthcare unit in São Luís, Maranhão. Data were collected through the administration of a not validated questionnaire and a clinical examination at the dental office. The outcome was oral health self-perception and the independent variables were age, gender, ethnicity, marital status, schooling, monthly household income, dental treatment, the conclusion of treatment, last type of service used, toothache in the previous six months, untreated dental caries, missing teeth, the DMFT index, root caries and removable partial denture. Descriptive statistics and the chi-square tests were performed with a 5% level of significance. Results: The sample was composed by 129 adults aged 25 to 55 years. The female gender (80.6%), brown skin color (62.8%) and low income (55.8%) were the most prevalent independent variables. Ninety-three percent of the sample had undergone some type of dental treatment, but only 36.4% concluded treatment. Seventy-nine percent perceived their oral health as negative. No significant associations were found between a negative self-perception and the independent variables analyzed. Conclusion: Most of surveyed individuals had a negative self-perception of their oral health, however, the perception was not associated with any of the exploratory variables.
Keywords: adults; self-concept; oral health.
Introduction
The health self-perception is the interpretation that one individual has about his/her health 1, scoring a quality degree from satisfaction to necessities. This evaluation is essential because the people's behavior is conditioned by this perception 7. In the context of the oral health, this evaluation is associated with the general health and the behaviors involving the health care 5. A negative self-perception may indicate the presence of oral problems due to the lack of health care, inadequate care or lack of information on oral health 2.
Studies evaluating the oral health self-perception of adolescents, young adults, and the elderly shows that the negative self-perception is related to the clinical, social, and economic factors. Factors as low educational level, unemployment, long period since the last dental appointment, treatment requirements, lost teeth, dry mouth, and difficulty in eating are related to the negative self-perception 6,8,12-14. Other studies found that the positive oral health self-perception is associated with low ages, high income, higher educational level, low DMFT index and small time elapsed since the last appointment 4,11.
The oral health self-perception is a fundamental question, together with a normative assessment to guide the public politics 16. The subjective vision enable the health managers to evaluate comprehensively the needs and allow the planning of actions for oral health care 4.
Considering that different cultural aspects may result in different health self-perception 4, this study aimed to evaluate the oral health self-perception of adults treated at a primary healthcare unit and the factors interfering on these perceptions.
Material and methods
This study was submitted and approved by the Institutional Review Board regarding to ethical aspects (protocol #854.682/2014). All patients read and signed a Free and Clarified Consent Form.
This cross-sectional study was performed from June /2014 to September/2014 with individuals attending to the primary healthcare unit in the city of São Luís, Maranhão, Brazil. The individuals were asked to participating into the study in the waiting room. Those who met the inclusion criteria read and signed the free and clarified consent form. The inclusion criteria comprised: adults, attending the primary healthcare unit for other appointments (not the dentist), not edentulous, without orthodontic appliance, and without mental and cognitive impairment.
The sample size was calculated by considering the main clinical condition investigated (dental caries). A prevalence of 95.5% of dental caries for the population aged between 35 and 44 years, of the city of de São Luís – MA 3. With a level of confidence of 95%, a power of 80%, and standard error of 5%, the minimum sample size was 134 individuals. No adjustment for the finite population was executed because the information about the number of individuals attending the healthcare unit during the study period could not be obtained.
A questionnaire was applied through interview by the researcher N.P.V. This quest ionnaire comprised demographic socioeconomic data, use of the dental services, self-reported oral morbidity (tooth pain in the last six months) and oral health self-perception (satisfaction with teeth/mouth, with the following answer options: "very satisfied"; "satisfied"; "nor satisfied neither dissatisfied"; "dissatisfied"; "very dissatisfied"). This variable was the study outcome, and dichotomized into positive "very satisfied" and "satisfied") and negative ("nor satisfied neither dissatisfied"; "dissatisfied"; and "very dissatisfied").
The clinical examination was carried out in a dental office inside the healthcare unit, under the light of the dental chair, with the aid of dental mirror, WHO probe, and gauze 18. The data collection followed all the biosecurity criteria with gloves, glasses, mask, cap, and disposable apron. The clinical data was collected regarding crown and root caries, restored and lost teeth, removable partial denture (RPD) (provisional or definitive)18.
A pilot study was conducted with 34 individuals to test the study methodology (application of the questionnaire and clinical examination) and calibrate the examiner for the DMFT index (K = 0.911). The data of this pilot study was not used in this main study.
The Statistical Package for the Social Sciences (SPSS, version 21.0, IBM Corporation, Armonk, New York, USA) was used for analyzing the data, including the descriptive analyses and chi-square test, at the level of significance of 5%.
Results
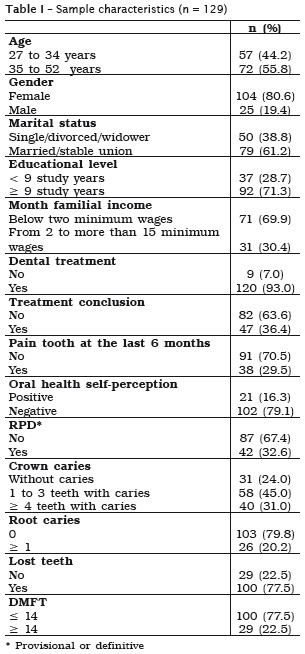
Of 489 individuals invited to participate in the study, 355 did not meet the inclusion criteria and five refused in participating. Thus, the response rate was of 96.3%. The studied convenience sample was composed by 129 individuals aged between 25 and 55 years, 80.6% females, 62.8% white. The month familial income was below two minimum wages for 69% of the sample. Individuals married or in stable union were 61.2% of the total sample. The negative oral health self-perception was 79.1% (table I).
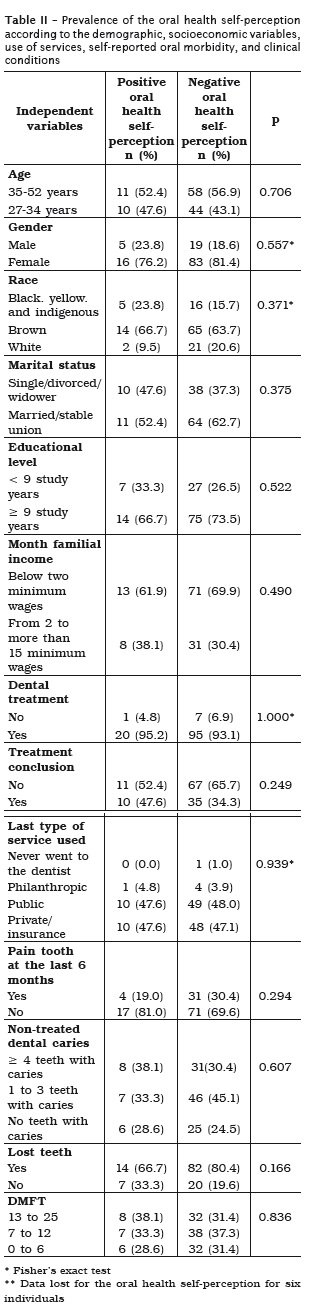
For the studied sample, no independent variable was associated with the outcome (table II).
Discussion
Most of the studied individuals (79.1%) showed negative oral health self-perception, a result different from other study on similar age range with a negative oral health self-perception of 33.2% 8. The different prevalence can be explained by the different socioeconomic conditions of different areas. While this present study was conducted in a Northeastern city of Brazil, with unfavorable socioeconomic situation for most of the population, the study of Luchi et al.. 8 was conducted in a Southern city of Brazil, with one of the highest indexes of human development among the Brazilian cities.
Although the low socioeconomic conditions are provenly associated with the negative oral health self-perception 6,8,13,14, in the present study, a significant association between income and negative self-perception did not occur, even with 69.9% of the individuals dissatisfied with the oral health received below two minimum wages. This lack of association may be related to the small sample size.
The Brazilian Unified Health System has basic principles as integrality and hierarchy that at most times are not fulfilled because of a small oriented management. Many times, the clientelism and the polarization of the oral health services rupture with the unified health system equity, resulting in difficulty in accessing the dental treatments10. Even those who has access may not have all the treatment requirements satisfied. Of the individuals with negative oral health self-perception, 48% searched for public dental treatment, which was expected, because 69.9% had an income below two minimum wages.
Economically vulnerable individuals tend not to search the dental treatment. When they do search, most of time, they did not complete the treatment. In this present study, most of the individuals with negative oral health self-perception already had undergone dental treatment (93.1%). However, 34.3% concluded the treatment. This pointed out that the treatment conclusion does not assure the satisfaction with either dental services or oral health.
In this present study, the individuals aged between 35 and 52 years were more dissatisfied with the oral health than those aged between 27 and 34 years. While some studies agree with these findings indicating that the oldest individuals had a more negative oral health self-perception 12,13, other studies observe the contrary result. In a research performed with elderly aged from de 60 years, in which most (54.5%) of the participants were classified into low socioeconomic level, the oral health self-perception was considered as positive, even in low conditions of oral health. Even with signs and symptoms of pain, difficult in mastication, appearance impairment, the health perception of the elderly is affected by the belief that some pain and impairments are natural of the aging process 7,17. This characteristic, so-called resignation, was also found in a study conducted in a Brazilian metropolis with 45 institutionalized elderlies from different social classes. Many faced the limitations as aging consequences and not as a problem to be corrected 6.
This study found that the individuals were dissatisfied with the oral health, suggesting that the found clinical conditions accounted for the negative perception. It is worth noting that a considerable percentage of the sample showed dental caries (76%) and 77.5% exhibited teeth lost.
This study exhibited some limitations, such as the convenience sample that impairs the extrapolation of the findings to the target population; and the small sample size that did not allow verifying the associations already proven by populationalbased studies. Moreover, because this is a crosssectional study, a cause-effect relationship could not be established. Thus, further studies are necessary to verify the oral health self-perception of these population whose socioeconomic conditions are known to be precarious. Studies with longitudinal design will enable to evaluate the provided public services.
Conclusion
Most of the studied individuals showed a negative oral health self-perception. However, the self-perception was not associated with none of the studied exploratory variables.
References
1. Bailis DS, Segall A, Chipperfield JG. Two views of self-rated general health status. Soc Sci Med. 2003 Jan;56(2):203-17. [ Links ]
2. Braga APG, Barreto SM, Martins AM. Autopercepção da mastigação e fatores associados em adultos brasileiros. Cad Saúde Pública. 2012 May;28(5):889- 904.
3. Brasil. Ministério da Saúde. Secretaria de Atenção à Saúde. Secretaria de Vigilância em Saúde. Departamento de Atenção Básica. Coordenação Geral de Saúde Bucal. Projeto SB BRASIL 2010. Pesquisa Nacional de Saúde Bucal – resultados principais. 2011. 92 p.
4. Cruz GD, Galvis DL, Kim M, Le-Geros RZ, Barrow S-YL, Tavares M et al.. Self-perceived oral health among three subgroups of Asian-Americans in New York city: a preliminary study. Community Dent Oral Epidemiol. 2001;29(2):99-110.
5. Gift HC, Atchison KA, Drury TE. Perceptions of the natural dentition in the context of multiple variables. J Dent Res. 1998;77(7):1529-38.
6. Haikal D, Paula AM, Martins AM, Moreira A, Ferreira E. Autopercepção da saúde bucal e impacto na qualidade de vida do idoso: uma abordagem quanti-qualitativa. Ciên Saúde Colet. 2011 Jul;16(7):3317-29.
7. Kiyak HA. Age and culture: influences on oral health behavior. Int Dent J. 1993;43(1):9-16.
8. Luchi CA, Peres KG, Bastos JL, Peres MA. Desigualdades na autoavaliação da saúde bucal em adultos. Rev Saúde Pública. 2013 Aug;47(4):740-51.
9. Martins AM, Barreto SM, Pordeus I. Fatores relacionados à autopercepção da necessidade de tratamento odontológico entre idosos. Rev Saúde Pública. 2008 Jun;42(3):487-96.
10. Martins RJ, Moimaz SAS, Garbin CAS, Garbin AJI, Lima DC. Percepção dos coordenadores de saúde bucal e cirurgiões-dentistas do serviço público sobre o Sistema Único de Saúde (SUS). Saúde Soc. 2009 Mar;18(1):75-82.
11. Matos DL, Lima-Costa MF. Autoavaliação da saúde bucal entre adultos e idosos residentes na região sudeste: resultados do Projeto SB-Brasil 2003. Cad Saúde Pública. 2006;22(8):1699-707.
12. Mendonça HLC, Szwarcwald CL, Damacena GN. Autoavaliação de saúde bucal: resultados da Pesquisa Mundial de Saúde – Atenção Básica em quatro municípios do estado do Rio de Janeiro, Brasil, 2005. Cad Saúde Pública. 2012 Oct;28(10):1927-38.
13. Molarius A, Engström S, Flink H, Simonsson B, Tegelberg A. Socioeconomic differences in self-rated oral health and dental care utilisation after the dental care reform in 2008 in Sweden. BMC Oral Health. 2014 Nov;14:134.
14. Olutola BG, Ayo-Yusuf AO. Socio-environmental factors associated with self-rated oral health in south Africa: a multilevel effects model. Int J Environ Res Public Health. 2012 Oct;9(10):3465-83.
15. Pauleto ARC, Pereira MLT, Cyrino EG. Saúde bucal: uma revisão crítica sobre programações educativas para escolares. Ciên Saúde Colet. 2004;9(1):121-30.
16. Silva RCS, Fernandes RAC. Autopercepção das condições de saúde bucal por idosos. Rev Saúde Pública. 2001;35(4):349-55.
17. Vasconcelos LCA, Prado Júnior RR, Teles JBM, Mendes RF. Autopercepção da saúde bucal de idosos de um município de médio porte do nordeste brasileiro. Cad Saúde Pública. 2012 Jun;28(6):1101-10.
18. World Health Organization – WHO. Oral health surveys. Basic methods Geneva. 1997.
 Corresponding author:
Corresponding author:
Nicole Paiva Veras
Rua Cumã, n. 12, Ed. Vega
Renascença II
CEP 65075-700
São Luís – MA – Brasil
E-mail: npaivaveras@gmail.com
Received for publication: May 9, 2016
Accepted for publication: November 22, 2016
