










Serviços Personalizados
Artigo
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRSBO (Online)
versão On-line ISSN 1984-5685
RSBO (Online) vol.14 no.1 Joinville Jan./Mar. 2017
ORIGINAL RESEARCH ARTICLE
Dentofacial deformity and quality of life: a case control study
Marcelo Carlos Bortoluzzi I; Cintia Cella I; Suelen Franke Haus I
I State University of Ponta Grossa – Ponta Grossa – PR – Brasil
ABSTRACT
Introduction: Dentofacial deformity (DFD) may be defined as facial and dental disproportions great enough to affect significantly the individual's quality of life (QoL). Objective: This study aimed to verify and compare the impacts of and differences in QoL in individuals with and without DFD. Material and methods: The impact of DFD on QoL was evaluated through the following questionnaires: Short Form Health Survey (SF36), a generic Oral Health Related Quality of Life (OHRQoL) questionnaire (Oral Health Impact Profile Questionnaire – OHIP-49), a condition-specific questionnaire for DFD (Orthognathic Quality of Life Questionnaire – OQLQ) and a single question answered by Visual Analogue Scale (VAS). Results: Greater and negative impacts on QoL were observed in patients with DFD in all domains of OQLQ and OHIP; and in two domains of SF36: emotional well-being and social functioning. Conclusion: DFD greatly and negatively impacted on QoL of individuals with DFD greater mainly evidenced through general and specific OHRQoL questionnaires.
Keywords: dentofacial necessity; oral health related quality life; dental care.
Introduction
The World Health Organization (WHO) defines QoL as "the perception of the individual and your position in life in the context of culture and value system in which he/she lives and about his/her goals, expectations and interests". QoL is a broad concept that can include the condition of physical and psychological health, the level of independence and social relationship 16. The dentofacial deformity (DFD) is the dental and facial disproportions large enough to significantly affect the QOL of an individual. It is considered that this population has a functional and/or socially disability, due to their dental and facial components are far from normal, which can affect some everyday situations. These individuals have difficulty in feeding in public because of their facial appearance 14, have low self-esteem and no self-confidence 15. Both the oral function, appearance, and interpersonal relationships impacts on QoL which have also been highlighted by other authors 1,2,11.
The DFD is characterized among the three Angle's malocclusion types. To classify the malocclusion, it is necessary to have a concept of normal occlusion. Occlusion is defined for the purposes of classification, as a frequency distribution with a range of aspects typically found in Classes I, II and III. The Angle's system is based on the anterior-posterior relationship of the jaws, and it is the more traditional, practical and therefore the most popular classification method in use. The Class I molar relationship is the normal positon (neutral occlusion) and therefore without DFD. Malocclusions in which there is a distal relationship of the mandible in relation to the maxilla are classified as Class II. Class II malocclusion is subdivided into Division 1 and Division 2. In Class II Division 1, the distal occlusion typically has the upper incisors in extreme labial version, usually with mouth breathing. In Class II Division 2 comprises the distal occlusion of the molars and the upper central incisors are at labially, almost normal or slightly lingual version, while the upper lateral incisors are labially or mesially tipped. The Class III malocclusion is the mesial of the mandible in relation to the maxilla. This malocclusion type is characterized by DFD 10.
Among the instruments for QOL measurement in Dentistry, OHIP-49 questionnaire measured the social impact of oral disorders. However, the instruments developed for Oral Health Related Quality of Life (OHRQoL) assessment tend to be designed for the assessment of the elderly. A specific instrument was developed and validated for assessing QOL in patients with DFD, as well as to verify the results of orthognathic surgery in the correction of the deformity, a questionnaire so-called Orthognathic Quality of Life Questionnaire (OQLQ) 4,5.
The OQLQ has four main components related to: social aspects of deformity, facial aesthetics, oral function and DFD self-perception 9. In this study, we compared two samples, totaling 106 respondents: 53 individuals with some degree of DFD, classified as Angle's Class II or Class III (23 males and 30 females), and 53 individuals without DFD, classified Angle's Class I (23 males and 30 females). All individuals answered the OQLQ, OHIP-49, SF-36 and VAS questionnaires.
This study aimed to verify and compare the QoL between individuals with (cases) and without DFD but with routine dental needs (controls), totalizing 106 participants.
Material and methods
This study was approved by the local Ethics Committee in Research (UNOESC/HUST) and aimed to compare the impact of QoL among patients with and without DFD by the following instruments: SF-36, OHIP-49, OQLQ and a single question answered through VAS.
We interviewed individuals with DFD who are in search of dental treatment, orthodontic treatment or a specific DFD treatment, and individuals without DFD matched by gender and age. For the sample of individuals with DFD, the inclusion criteria were presence of DFD and all teeth. The exclusion criteria were DFD individuals previously submitted to orthognathic surgery, with syndromes or congenital deformities, for example, cleft lip and palate, and deformity or sequela from severe face trauma. The exclusion criteria for the control group was presence of DFD, users of orthodontic device, removable and total dentures, absence of 4 or more teeth without replacement by implants/fixed dentures. The control sample was composed only by patients with Angle Class I malocclusion, with all teeth or with loss of up to 4 teeth replaced by fixed prostheses/implants. Patients who were invited to participate responded to the questionnaires after a full explanation about the objectives of the research. Instructions on how to respond to questionnaires were delivered to patients and any questions on the issues could be solved by a research assistant.
The OQLQ consists of 22 items on a scale of 4 rating points as follows: 1 = "bothers a little"; 2 = do not bother; 3 = not applicable; 4 = "very bothering". The 22 items are divided into: social aspects of deformity (first component), facial aesthetics (second component), oral function (third component) and consciousness of DFD (fourth component). The OQLQ score is performed by adding individual items within the domains. The total score OQLQ can vary between 0 and 88, including the specifically domains, as follows: social aspects of deformity, 0-32; facial aesthetics, 0-20; oral function, 0-20; and awareness of the DFD, 0-16. A higher score indicates worst QoL and a lowest score a better QoL 3,5,8.
The OHIP-49 questionnaire is an instrument of 49 questions designed to measure how much oral conditions affect the QoL in a general sense. OHIP is organized into seven dimensions: functional limitations, physical pain, psychological discomfort, physical disabilities, psychological incapacity, social disability and disability. OHIP-49 criteria vary from 0-40, and the values are obtained by means of a weighted average of the questions. Higher scores indicate a worse OHRQoL 13.
The Brazilian version of SF-36 consists of 36 items divided into eight areas: functional capacity, physical aspects, pain, general health, vitality, social, emotional and mental health performance. For each subscale, the raw data are transformed to a 0-100 scale, in which a high score indicates better result 9,12. VAS varies from 0-100, with higher scores indicate better QoL. This Likert scale of single response reports information and generic QoL concepts and, after reading, the patient chooses by indicating a point on the scale that best describes the current QoL. Data were analyzed through the statistical software STATA 8.0.
In the OQLQ survey, the social aspects of deformity are assessed on items 15 to 22; facial aesthetics in items 1, 7, 10, 11, 14; oral function in items 2 to 6; the answers of the DFD, items 8, 9, 12 and 13; the answers were summed to obtain the total score. The OHIP-49 questionnaire consists of sections and among them each answer given to question must be multiplied by a certain specified amount (weight): ▪ functional limitation (OHIP1 * 1.253 + OHIP2 * 1.036 + OHIP3 * 0.747 + OHIP4 * 1.059 + OHIP5 * 1.154 + OHIP6 * 0.931 + OHIP7 * 1.181 + OHIP8 * 1.168 + OHIP17 * 1.472); ▪ physical pain (OHIP9 * 1.213 + OHIP10 * 0.937 + OHIP11 * 1.084 + OHIP12 * 1.053 + OHIP13 * 1.361 + OHIP14 * 1.088 + OHIP15 * 0.998 + OHIP16 * 1.264 + OHIP18 * 1.002); ▪ psychological discomfort (OHIP19 * 2.006 + OHIP20 * 1.902 + OHIP21 * 2.252 + OHIP22 * 1.815 + OHIP23 * 2.025); ▪ physical impairment (OHIP24 * 1.109 + OHIP25 * 1.111 + OHIP26 * 1.051 + OHIP27 * 1.068 + OHIP28 * 1.266 + OHIP29 * 1.022 + OHIP30 * 1.351 + OHIP31 + 1.070 + OHIP32 * 0.952); ▪ psychological impairment (OHIP33 * 1.950 + OHIP34 * 1.393 + OHIP35 * 1.646 + OHIP36 * 1.936 + OHIP37 * 1.638 + OHIP38 * 1.437); ▪ social impairment (OHIP39 * 1.572 + OHIP40 * 2.555 + OHIP41 * 1.832 + OHIP42 * 2.236 + OHIP43 * 1.805); ▪ incapacity (OHIP44 * 2.112 + OHIP45 * 1.420 + OHIP46 * 1.545 + OHIP47 * 1.567 + OHIP48 * 1.879 + OHIP49 * 1.476). The total is represented by the sum of all the areas already multiplied by its pre-set values and divided by seven domains.
The SF-36 questionnaire has eight sections: physical function evaluated (items 3 to 12); limitations to physical efforts (items 13 to 16); emotional problems (items 17 to 19); energy/fatigue (items 23, 27, 29 and 31), emotional (items 24, 25, 26, 28 and 30); social function (items 20 and 32); pain (items 21 and 22) and general health (items 1, 33, 34, 35, 36). Certain weights are established for each response. For questions number 1, 2, 20, 22, 34 and 36 answers have weight 100; number 2 weight 75; number 3 weight 50; number 4 weight 25; and number 5 weight 0. For questions number 3 to 12 responses equal to number 1 have weight 0, number 2 weight 50 and number 3 weight 100. The questions number 13 to 19 only have as options the number 1 and 2, with weight 0 and 100, respectively. For the questions number 21, 23, 26, 27 and 30 possible answers are 1 to 6: number 1 = weight 100, number 2 weight 80, number 3 weight 60 and so on, decreasing 20, until the responses of number 6 have weight equal to 0. For the 24, 25, 28, 29 and 31 of the possible answers are also from 1 to 6, but in these the responses number 1 has weight 0, and each number increase 20 points, so the answer number 6 have weight 100. And the questions number 32, 33 and 35 can be answered from 1 to 5, where 1 has weight 0; 2 weight 25; 3 weight 50; 4 weight 75; and 5 weight 100. VAS requires only that the respondent assesses the overall QoL, and the number 0 indicates the worst and 100 the best QoL possible from 0 to100.
Results
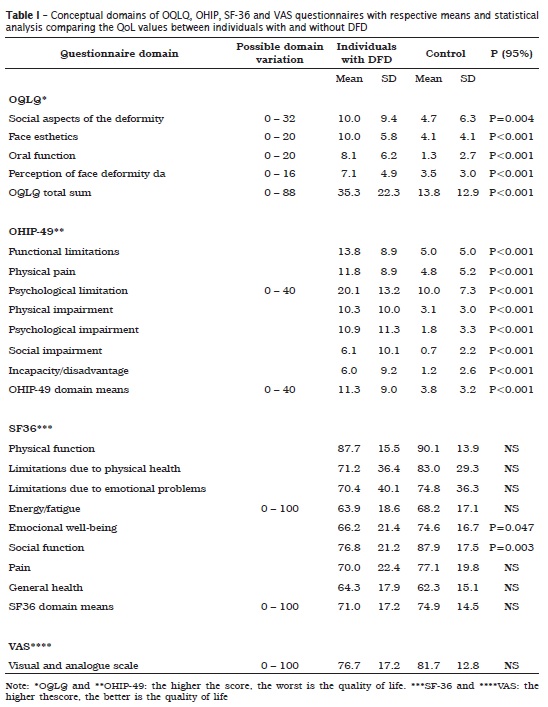
The descriptions according to the OQLQ, OHIP-49, SF-36 and VAS domains with their impacts on QOL for individuals with DFD and controls, are summarized in table I.
Discussion
This study aimed to verify and compare the QoL between two groups of individuals, with (cases) and without DFD (controls), through three questionnaires (OQLQ, OHIP-49, SF-36) and a single question answered by VAS. Few studies comprehensively evaluated the QoL of individuals with DFD as this present study.
The results of the present study indicated that, for OHRQoL questionnaires, there was a significant and negative impact for all the domains of OQLQ and OHIP questionnaires, indicating that the DFD interferes in the psychological, physical, symptomatologic, and functional contexts, as well as influences on the social activity of the individual, in comparison with the individuals without DFD. Interestingly, the impacts were not generalized and expressed in the generic QoL questionnaire, except for the domains related to emotional well-being and social function, which had expressed the broader impact on ORHQoL. These differences between generic and specific questionnaires can be explained by the nature of the questions either directed to the problem or taken broadly, which corroborates the suggestion of the use of different questionnaires 1. However, the question of interpretation still remains when one questionnaire evidences the impact/limitation but the general questionnaire does not.
A case-control study (individuals with or without deformity), assessed the QoL of individuals with DFD (n=143) - 36 before orthognathic surgery, 35 after orthognathic surgery, 35 who refused to undergo orthognathic surgery and 37 controls. The QoL was assessed by applying the OQLQ and SF-36 questionnaires. The pre-surgical results were similar to those found in this present study with negative and significant impacts for all areas of OQLQ. The comparison between the OQLQ of a Jordanians study 1 showed total OQLQ scores similar to those of the present study: Jordanians with DFD -38 Brazilians with DFD -35; and Jordanians and Brazilians without DFD - 13. The SF-36 means were also very similar, with overall average for Jordanians (72) and Brazilians (71) with DFD; Jordanians (70), and Brazilians (75) without DFD. It is worth noting the similar results of impacts and measures of OQLQ and SF-36 despite of the cultural difference between two populations 1.
The depression could be linked to individuals with DFD and may interfere significantly on vitality, social aspects of the individual and mental health. Studies shows that non-treated DFD may result in low self-esteem and negative impact on social life, including social restrictions 6.
A study investigated the relationship between negative impacts on daily performance due to malocclusion and psychological stress in healthy nonsmoking Japanese adults aged between 18 and 19 years. The sample was composed by 641 individuals (329 male and 312 female); of these, 255 individuals had malocclusion. The individuals with malocclusion had a negative impact in relation to those without malocclusion. The psychological stress and depression were significantly correlated to malocclusion. Therefore, negative impacts on daily performance due to malocclusion can contribute to psychological stress in Japanese adults 7.
Another study evaluated two groups before and after treatment, using SF-36 and OQLQ. One group comprised individuals with squared face or prominent zygomatic; the other group was submitted to treatments. SF-36 found significant difference in physical function and body pain (P<0.05) at pre-treatment between the two groups. At pre-treatment, no significant differences were found in oral function and face esthetics of OQLQ (P<0.001), while at post-treatment, only the oral function domain showed significant difference. Therefore, the treatment had a positive impact on QoL, regardless of the type of deformity. The OQLQ showed better ability of distinction and could point out the subtle differences between the two groups 9.
Also, other authors assessed the impact and clinical significance of DFD treatment on QoL. Sixty-two individuals were examined (27 males and 35 females) aged 18-38 years. The data were collected by means of a measure of validated health status, through OQLQ and VAS at preoperative period. Six months after treatment, the questionnaires were applied again. After treatment, OQLQ scores improved for each domain (p<0.05). The proportion of patients reporting a moderate or great improvement was: facial appearance (93%), mastication function (64%), comfort (60%), and speech (32%). Clinical significance of changes of the scales has been reported in terms of effect sizes, and the greatest effect was in facial aesthetics. The clinical impact was moderate on social aspects of deformity and oral function and a small effect on consciousness of DFD. This research confirms that the treatment of the DFD can cause positive effects on QoL 11.
Conclusion
Patients with DFD had worst QoL than patients without DFD and need of routine dental needs, primarily evidenced by general and specific OHRQoL instruments.
References
1. Al-ahmad HT, Al-sa'di WS, Al-omari IK, Al-bitar ZB. Condition-specific quality of life in Jordanian patients with dentofacial deformities: a comparison of generic and disease-specific measures. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009;107(1):49-55. [ Links ]
2. Bock JJ, Odemar F, Fuhrmann RA. Assessment of quality of life in patients undergoing orthognathic surgery. J Orofac Orthop. 2009;70(5):407-19.
3. Bortoluzzi MC, Manfro R, Soares IC, Presta AA. Cross-cultural adaptation of the orthognathic quality of life questionnaire (OQLQ) in a Brazilian sample of patients with dentofacial deformities. Med Oral Patol Oral Cir Bucal. 2011;16(5):e694-9.
4. Cunningham SJ, Garrat AM, Hunt NP. Development of a condition-specific quality of life measure for patients with dentofacial deformity: I. Reliability of the instrument. Community Dent Oral Epidemiol. 2000;28(3):195-201.
5. Cunningham SJ, Garratt AM, Hunt NP. Development of a condition-specific quality of life measure for patients with dentofacial deformity: II. Validity and responsiveness testing. Community Dent Oral Epidemiol 2002;30(2):81-90.
6. De Ávila ED, De Molon RS, Loffredo LCM, Massucato SEM, Vieira EH. Health-related quality of life and depression in patients with dentofacial deformity. Oral Maxillofac Surg. 2013;17(3):187-91.
7. Ekuni D, Furuta M, Irie K, Azuma T, Tomofuji T, Murakami T et al. Relationship between impacts attributed to malocclusion and psychological stress in young Japanese adults. European Journal of Orthodontics. 2011;33(5):558-63.
8. Gava EC, Miguel JA, Araújo AM, Oliveira BH. Psychometric properties of the Brazilian version of the Orthognathic Quality of Life Questionnaire. J Oral Maxillofac Surg. 2013;71(10):1762.e1-8.
9. Khadka A, Liu Y, Li J, Zhu S, Luo E, Feng G et al. Changes in quality of life after orthognathic surgery: a comparison based on the involvement of the occlusion. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2011;112(6):719-25.
10. Moyers RE. Ortodontia. 4. ed. Rio de Janeiro: Guanabara Koogan; 1991.
11. Murphy C, Kearns G, Sleeman D, Cronin M, Allen PF. The clinical relevance of orthognathic surgery on quality of life. Int J Oral Maxillofac Surg. 2011;40(9):926-30.
12. Nicodemo D, Pereira MD, Ferreira LM. Effect of orthognathic surgery for class III correction on quality of life as measured by SF-36. Int J Oral Maxillofac Surg. 2008;37(2):131-4.
13. Pires CP, Ferraz MB, Abreu MH. Translation into Brazilian Portuguese, cultural adaptation and validation of the oral health impact profile (OHIP-49). Braz Oral Res. 2006;20(3):263-8.
14. Proffit WR, White RP, Sarver DM. Contemporary treatment of dentofacial deformity. St. Louis: Mosby/Elsevier Science; 2003.
15. Soh CL, Narayanan V. Quality of life assessment in patients with dentofacial deformity undergoing orthognathic surgery – a systematic review. Int J Oral Maxillofac Surg. 2013;42(8):974-80.
16. Study protocol for the World Health Organization project to develop a quality of life assessment instrument (WHOQOL). Qual Life Res. 1993;2(2):153-9.
 Corresponding author:
Corresponding author:
Marcelo C. Bortoluzzi
Departamento de Odontologia
Faculdade de Odontologia, bloco M
Av. General Carlos Cavalcanti, 4748 – Uvaranas
CEP 84.030-900 – Ponta Grossa
Paraná – Brasil
E-mail: mbortoluzzi@gmail.com
Received for publication: June 9, 2015
Accepted for publication: March 7, 2017
