










Serviços Personalizados
Artigo
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRSBO (Online)
versão On-line ISSN 1984-5685
RSBO (Online) vol.14 no.1 Joinville Jan./Mar. 2017
ORIGINAL RESEARCH ARTICLE
Knowledge of dentists on child abuse in two Brazilian southern cities
Cintia Rejane da Silveira de Mello I; Leticia Brandalise Moletta I; Carolina Dea Bruzamolin I; Marilisa Carneiro Leão Gabardo I; Eduardo Pizzatto I; Wellington Menirval Zaitter I
I Positivo University – Curitiba – PR – Brasil
ABSTRACT
Introduction: The child abuse against children and teenagers is relevant and the dentist has a fundamental role in the process of identification of suspected cases. Objective: To evaluate the level of knowledge of the dentists about child/teenager abuse and the attitude towards identified cases, in the cities of Rio Negro (Paraná, Brazil) and Mafra (Santa Catarina, Brazil). Material and methods: Questionnaires were applied to 44 professionals of these cities, who practiced in private and/or public health service. The questions covered the profile of respondents regarding gender, institution (public or private), level of education, practicing time and place. The information on abuse comprised the level of information about violence and knowledge on the compulsory notification of suspected cases. Results: Regarding the cases of abuse, 34% of the sample dealt with this situation. Almost half of respondents (47.7%) reported being able to recognize the typical lesions of child abuse, yet only 32% felt trained to do so. Only 22.7% reported having training to detect suspected cases. And 91% said they would notice the Guardian Council. About 48% confirmed they had knowledge of the legal implications in case of omission. Conclusion: Most of the dentists had insufficient knowledge about child abuse. However, the dentists know how to deal with such a situation. Continuing education seems to be an appropriate strategy to promote professional knowledge on the subject. It is also suggested the implementation of a national protocol to facilitate notifications and the classification of abuse types.
Keywords: Forensic Dentistry; child abuse; questionnaire.
Introduction
Abuse against children and adolescents can be practiced by omission, by deletion or by transgression of their rights, defined by legal conventions or cultural norms 23.
Based on the data of the Registry of Human Rights of the Presidency of the Brazilian Republic, in 2013, through Right Human Dialing (dials 100), it was registered 182,880 complaint on restrictions of rights; of these, 124,079 were on adolescent and children 6.
Some studies demonstrate that most of the injury caused by child abuse involves the region of head and neck. In addition, often the individual who suffered the aggression is taken to seek dental treatment. These aspects put the dentist in a position to identify the victims 15.
As major orofacial lesions are: bruises, lacerations of oral mucosa, lip, palate, gingiva; mouth opening deviation; presence of bed sores in the corners of the mouth in case of gagged children; burns on the gums, tongue or palate mucosa caused by hot food or household items; and bruises on cheeks 24.
In Brazil, the dentist, as citizen, has the legal, ethical and moral duty to notify to the competent authorities (Tutelary Council) the cases suspicious of abuse based on the Federal Constitution and in the Statute of the Child and Adolescent (ECA) 27.
The dentist's unpreparedness in dealing with victims of abuse should occur due to ignorance about how to proceed against these cases, even in graduation the issue is irrelevant 2. In addition, in Brazil, there are several barriers against the notification such as: shortage of regulations for technical procedures, the absence of legal protection mechanisms to the professionals who notified, fail in identifying the violence in the health service and break in the professional secrecy 18.
Therefore, this study aimed to verify the level of knowledge of dentists about child abuse, in the cities of Mafra (SC) and Rio Negro (PR).
Material and methods
This study was developed in the cities of Mafra (SC) and Rio Negro (PR). The estimated population of the two cities together is of approximately 87,000 inhabitants 4. The separation between localities is given by the Rio Negro, which allows to consider them "sister cities".
This exploratory, descriptive cross-sectional study employed a not probabilistic sample of 50 dentists, from both cities. The information was obtained through a questionnaire with closed questions about the dentist's profile (gender, public or private institution, practice time and place), knowledge about the characteristics that identify abuse, and if so, where this knowledge was acquired, the experience in these cases, the attitude adopted during the suspicious situation, the recognition of responsibility in reporting as health professional, in which place/institution to report and, finally, the legal implications.
Together with the questionnaire an explicative letter on the purpose of the research was sent, to facilitate the agreement of the dentist regarding the importance of its contribution. The participants' confidentiality was assured.
The obtained data was tabulated in frequency for better visualization and understanding, using Statistical Package for Social Sciences software (SPSS), version 19.0.
Results
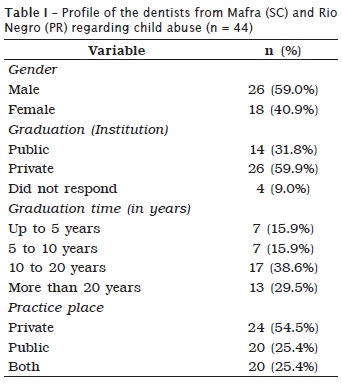
Forty-four dentists answered to the questionnaire, representing a response rate of 80%. Table I shows the data of the dentist's profile. Generally, most of the sample were males, graduated in in particular universities, with time of graduation between 10 and 20 years, and with private or public practice (table I).
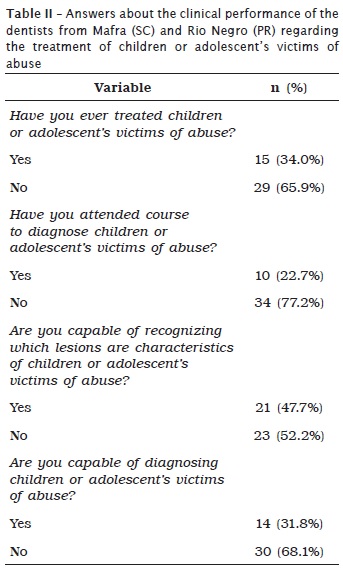
Approximately 50% of the dentists affirmed to be capable of recognizing which were the typical injuries of child abuse. However, most dentists did not received formation on the diagnosis of child/adolescent abuse. In its clinical performance, about 34% of the dentists had the chance to take care of children or adolescents victims of abuse (table II).
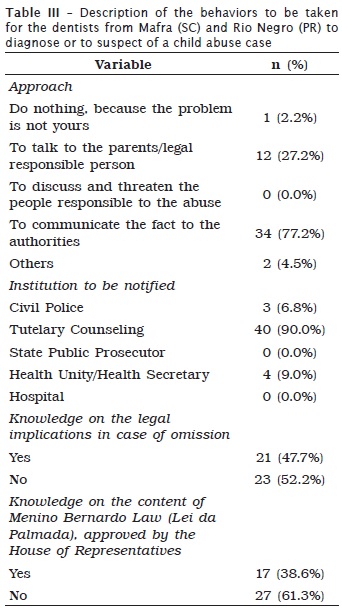
Facing a suspicious case of child abuse, the behavior of most dentist was to communicate the fact to the authorities; 90% would notify the Tutelary Council. The legal implications of this omission are known by almost half of the sample, but only 38% had knowledge on the content of the Menino Bernardo Law 16 (table III).
Discussion
Child abuse continues to be a threat to society that causes physical and emotional damage to the child, and these features, in many cases, affects the face 23. This research aimed to identify the level of knowledge of the dentists from two cities about child abuse.
Violence against children and adolescents is considered a public health issue, given the amount of complaints that reaches the Human Development Secretariat ultimately and that comes from all Brazilian municipalities. We also know that not all are notified, and it is believed that for every 20 situations of violence, only one is reported, according to ABRAPIA 1.
There are several forms of abuse against children and adolescents, and there are signs and symptoms that can help to prevent, diagnose or even act in suspected cases by the dentist 15.
In this study, 44 dentists, mostly males, responded to the questionnaire in time. Mostly of the dentists worked in private practice and were graduated for more than ten years, in private institution.
In relation to the ability to diagnosis child/teenager abuse, only 23% of the sample claimed they have received information on the subject. In the study of Santos et al. 20, conducted with Pediatric Dentists from Uberlândia and Araguari, in Minas Gerais, 90% of the participants had received information on child abuse. Tornavoi et al. 25, in their research with random sample of 180 questionnaires distributed between dentists graduated in the period from 1998 to2009, by the School of Dentistry of Ribeirão Preto, had evidenced that 39% of the interviewed dentists had not received instruction on question of domestic violence against children during the graduation. For Souza et al. 24, 90% of the undergraduates reported to be instructed during the graduation on the subject, and of these, 20% had considered the content satisfactory. Biss et al. 2, in the analysis of the curriculum of the courses of graduation in Dentistry, in Brazil, concluded that the subject has been little explored, although the relevance of the subject.
In the present research, almost half of the sample told to be capable to recognize the typical injuries of child abuse. For Silveira et al. 22, most of the dentists reported to be capable of diagnosing the physical damages, which corroborates the findings of Gomes et al. 11. Massoni et al. 15 conducted a literature search to identify the main aspects of orofacial child abuse and neglect, and confirmed the importance of the dentist in the recognition of orofacial changes caused by trauma or abuse in children, as well as the discrepancy between clinical findings and the story reported by the legal responsible, indicative of a suspected case.
With regards to the clinical practice, about 34% of the respondents in this study could assist children and adolescents' victims of abuse. Agreeing with these findings, Tornavoi et al. 25 found that 34% of the participants indicated the treatment to children suspected of abuse. Similar findings were observed by Fracon et al. 9, who observed that 26.31% of the participants suspected that some of their patients (children and/or teenagers) have suffered domestic or psychic violence. Silveira et al. 22 reported that 65% of the respondents reported never having attended children exposed to this type of violence, despite the high prevalence of the records in the archives of Legal Medical Institute of the places where the study was conducted.
As regards to training for the diagnosis of children or teenagers abused, it was observed that approximately 32% felt able to diagnose this type of abuse. This number increased in the study of Fracon et al. 9, in which 68.43% answered that they were capable to identify injuries from violence. 81.4% of the Dentistry undergraduates of the city of João Person answered that they have interest in receiving qualification for diagnosing abuse 24. Kaur et al. 13 evaluated the knowledge level and behavior of dentists after the identification of child abuse. The authors pointed out that 89.7% of the professionals are capable to distinguish accidental injuries from physical abuse; however, even that 50% knew their legal obligations in reporting, in many cases, they did not know how to report due to fear or lack of knowledge. The underreporting of child abuse is a significant problem for the dentist, so that instruction on the identification and notification of those cases are important to decrease the risk of the child to suffer new physical or emotional injuries 13.
In Netherlands, in 2012, the Dutch Association of Dentistry released a text-book on how the dentist will identify the signals of child abuse and act facing the situation of child abuse/neglect. The text-book considers the report of the dentist an obligation. van Dam et al. 26 questioned 1,038 dentists in the country about the use of the text-book, the identification and reporting of abuse cases. The results of the survey indicated that 80% of the respondents knew about the obligation to report the identified cases, but 81% filled in patient's records on the suspicion of child abuse and only 58% already did. It is seen that even with the existence of a text-book and guidance concerning the obligatory complaint, many professionals felt inhibited, and were not sufficiently informed about aspects of a case and which measures need to be taken.
The ECA states in article 245 that the healthcare professional is required by law to notify suspicious or confirmed situations of child abuse, with penalty from three to 20 reference wages, increased two-folded in cases of recurrence if the professional fails to communicate to the competent authority 5. The Tutelary Council is the institution responsible for guaranteeing the child/teenager rights. If the report to the Tutelary Council is not possible, the Court of Infancy and Youth must be communicated.
In accordance with Sales-Perez et al. 19, the law clearly states that it is the duty of every citizen, including the dentist, to report any suspicion or evidence of child abuse. The authors even mentioned that, although there is no specific chapter on the Brazilian Dentistry Ethics Code 7, the article 5, item V states the obligation to ensure the health and dignity of the patient; the item (VII), stresses the obligation to promote collective health in the performance of their duties, positions and citizenship, regardless of the public or private practice.
A questionnaire study, conducted in Fortaleza, analyzed the process of notification of child/teenager abuse by doctors, nurses and dentists of the family health program (PSF) and concluded that 64.4% of the sample could deal adequately with situations of violence, except for the dentists because 68.5% of them did not know the ECA and 60.80% did not know the notification sheet 14. In addition, Franzin et al. 10 identified in a systematic review on the subject, a wide variety of terms and types of violence, sometimes imprecise, which can lead to confusion about the classification of cases.
In this present study, when questioned on the conduct to be taken during the diagnosis or suspicion of child/teenager abuse, 77.3% of professionals answered that they would communicate the fact to the competent authorities. In the case, the Tutelary Council was the agency of election by 90.9%. However only half of the sample had knowledge on the legal implications that the dentist can suffer in case of omission. Fracon et al. 9 affirmed that all the participants would make the denunciation (100%), even so only 40% would communicate if they were sure about the abuse and 42% would notify the fact to the Tutelary Council. The same was verified by Silveira et al. 22, who found that a great number of professionals did not report the case, because of "uncertainty of the suspicion". Silva-Oliveira et al. 21, in experiment with 107 health professionals from Belo Horizonte observed that 56.1% of the respondents already faced child abuse cases, but only 28% had notified them to the authorities. Santos et al. 20 corroborated the fact that the dentist is legally obliged to report cases of child abuse (64.7%).
When examining the level of knowledge of the dentists, 83% of them working at public practice indicated to know how and to whom they report cases of abuse against children. In comparison with the data of this research, the rate of affirmative responses regarding the communication of cases to the Tutelary Council has reached 90% 8.
One of the reasons for this low level of complaints to the competent organs may be due to lack of information on the subject during graduation. Thus, there are indications that the subject should become part of the curriculum matrix, to alert the professional to combating child violence 27. It is necessary that the Federal Council of Dentistry (CFO) clarifies in the professional code of ethics, the conducts and duties to be taken by the dentist when facing child abuse 16.
Gomes et al. 12 showed that compared to the complexity of violence committed against children and adolescents, issues such as professional training, planning of integrated actions and professional participation in public actions should be balanced aiming to a better approach.
On this approach, they identified the need for a law regulating which effectively is considered child/teenager abuse. In this sense, the Law against Spanking, which prohibits physical punishment as a way of disciplining children and adolescents, was sanctioned and published in the Brazilian Official Diary of the Union on June 27, 2014 17. This law provides that family members, public officials and other people in charge of taking care of children who break the law will be referred to official or community program of family protection, psychological or psychiatric treatment and call to order. Yet, according to the text, the Union, the States and the municipalities shall act in an articulated manner in the development of public policy and implementation of actions aimed at preventing the use of physical punishment. In this study, 38.6% of the respondents stated they knew the content of this new law.
Further studies are necessary to clarify the level of knowledge on child abuse at populational level, because this study methodology did not allow such inference.
Conclusion
The studied dentist mostly had insufficient knowledge about child abuse, but they knew how to proceed facing that situation.
The continuing education can be a positive strategy to provide the professional's knowledge on the signs and symptoms of child abuse, as well as the role of the dentist, while health professional and citizen, in the treatment of victims. Still, it is suggested the implementation of a national protocol to facilitate the notifications and classifications of abuse types. Professional associations should raise awareness on the need for training and determination of changes in the code of ethics, with the mandatory inclusion of the topic in the course of dentistry at the different levels.
References
1. Associação Brasileira Multiprofissional de Proteção à Infância e à Adolescência – ABRAPIA. Guia de orientação para profissionais da saúde. 2. ed. Rio de Janeiro; 1997.
2. Biss SP, Duda JG, Tomazinho PH, Pizzatto E, Losso EM. Maus tratos infantis: avaliação do currículo dos cursos em odontologia. Rev ABENO. 2015;15(1):55-62.
3. Bohner LOL, Bohner OL, Canto GL. Maus-tratos da infância e adolescência: protocolo de atendimento no consultório odontológico. Rev Elet em Gestão, Educação e Tecnologia Ambiental. 2012; 6(6):1239-43.
4. Brasil. Instituto Brasileiro de Geografia e Estatística – IBGE. Cidades@ 2013 [cited 2014 Aug 5]. Available from: URL:http://www.cidades.ibge.gov.br/xtras/home.php.
5. Brasil. Lei n.° 8.069, de 13 de julho de 1990. Dispõe sobre o Estatuto da Criança e do Adolescente e dá outras providências. Diário Oficial da União; 16 Jul. 1990.
6. Brasil. Secretaria de Direitos Humanos da Presidência da República [cited 2014 Aug 5]. Available from: URL:http://www.sdh.gov.br/assuntos/criancas-e-adolescentes/dados-estatisticos.
7. Conselho Federal de Odontologia – CFO. Resolução n.° 118, de 11 de maio de 2012. Código de ética odontológica. Rio de Janeiro; 2012.
8. Dalledone M, Paola APB, Correr GM, Pizzatto E, Souza JF, Losso EM. Child abuse: perception and knowledge by Public Health Dentistry teams in Brazil. Braz J Oral Sci. 2015;14(3):224-9.
9. Fracon ET, Silva RHA, Bregagnolo JC. Avaliação da conduta do cirurgião-dentista ante a violência doméstica contra crianças e adolescentes no município de Cravinhos (SP). RSBO. 2011;8(2):153-9.
10. Franzin LCS, Franzin FM, Moysés ST. Violência doméstica contra crianças e adolescentes: prevalência em cidade do sul do Brasil. Colloquium Vitae. 2012;4(2):79-84.
11. Gomes LS, Pinto TCA, Costa EMMB, Ferreira JMS, Cavalcanti SDLB, G[ranville-Garcia AF. Percepção de acadêmicos de Odontologia sobre maus-tratos na infância. Odontol Clín Cient. 2011;10(1):73-8.
12. Gomes R, Junqueira MFPS, Silva CO, Junger WL. A abordagem dos maus-tratos contra a criança e o adolescente em uma unidade pública de saúde. Ciên Saúde Colet. 2002;7(2):275-83.
13. Kaur H, Chaudhary S, Choudhary M, Manuja N, Chaitra TR, Amit SA. Child abuse: cross-sectional survey of general dentists. J Oral Biol Craniofac Res. 2016;6(2):118-23.
14. Luna GLM, Ferreira RC, Vieira LJES. Notificação de maus-tratos em crianças e adolescentes por profissionais da Equipe Saúde da Família. Ciên Saúde Colet. 2010;15(2):481-91.
15. Massoni ACLT, Ferreira AMB, Aragão AKR, Menezes VA, Colares V. Aspectos orofaciais dos maus-tratos infantis e da negligência odontológica. Ciên Saúde Colet. 2010;15(2):403-10.
16. Matos FZ, Borges AH, Neto IM, Rezende CD, Silva KL, Pedro FLM et al. Avaliação do conhecimento dos alunos de graduação x cirurgião-dentista no diagnóstico de maus-tratos a crianças. Rev Odontol Bras Central. 2013;22(63):153-7.
17. Revista Consultor Jurídico [cited 2014 Aug 5]. Available from: URL:http://www.conjur.com.br/2014-jun-27/dilma-sanciona-lei-palmada-desobriga-servidor-denunciar-abuso.
18. Saliba O, Garbin CAS, Garbin AJI, Dossi AP. Responsabilidade do profissional de saúde sobre a notificação de casos de violência doméstica. Rev Saúde Pública. 2007;41(3):472-7.
19. Sales-Peres A, Silva RHA, Lopes-Júnior C, Carvalho SPM. Odontologia e o desafio da identificação de maus-tratos. Odontologia Clín Cient. 2008;7(3):185-9.
20. Santos JF, Nunes KS, Cavalcante AL, Silva EC. Maus-tratos infantis: conhecimento e atitudes de odontopediatras em Uberlândia e Araguari, Minas Gerais. Pesq Bras Odontoped Clín Integr. 2006;6(3):273-9.
21. Silva-Oliveira F, Ferreira EF, Mattos FF, Ribeiro MTF, Cota LOM, Vale MP et al. Adaptação transcultural e responsabilidade de questionário para avaliação de conhecimento e atitude de profissionais de saúde frente a caso de abuso físico infantil. Ciên Saúde Colet. 2014;19(3):917-29.
22. Silveira JLGC, Mayrink S, Nétto OBS. Maus-tratos na infância e adolescência: casuística, conhecimento e prática de cirurgiões-dentistas de Blumenau – SC. Pesq Bras Odontoped Clín Integr. 2005;5(2):119-26.
23. Sociedade Brasileira de Pediatria. Centro Latino-Americano de Estudos de Violência e Saúde Jorge Carelli. Escola Nacional de Saúde Pública. Secretaria de Estado dos Direitos Humanos. Ministério da Justiça. Guia de atuação frente a maus-tratos na infância e na adolescência: orientações para pediatras e demais profissionais que trabalham com crianças e adolescentes. 2. ed. Rio de Janeiro; 2001.
24. Sousa GFP, Carvalho MMP, Granville-Gracia AF, Gomes MNCG, Ferreira JMS. Conhecimento de acadêmicos em Odontologia sobre maus-tratos infantis. Odonto. 2012;20(4):101-8.
25. Tornavoi DC, Galo R, Silva RHA. Conhecimento de profissionais de Odontologia sobre violência doméstica. RSBO. 2011;8(1):54-9.
26. van Dam BAFM, van der Sanden WJM, Bruers JJM. Recognizing and reporting domestic violence: attitudes, experiences and behavior of Dutch dentists. BMC Oral Health. 2015;15:159.
27. Wacheski A, Lopes MGK, Paola APB, Valença P, Losso EM. O conhecimento do aluno de Odontologia sobre maus-tratos na infância antes e após o recebimento de uma cartilha informativa. Odonto. 2012;20(39):7-15.
 Corresponding author:
Corresponding author:
Marilisa Carneiro Leão Gabardo
Rua Professor Pedro Viriato Parigot de Souza, 5300
Campo Comprido
CEP 81280-330 – Curitiba
Paraná – Brasil
E-mail: marilisagabardo@gmail.com
Received for publication: December 12, 2016
Accepted for publication: March 7, 2017
