










Services on Demand
Article
 pdf in English
pdf in English Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailRelated links
Share

 Permalink
PermalinkStomatos
Print version ISSN 1519-4442
Stomatos vol.18 n.34 Canoas Jan./Jun. 2012
SCIENTIFIC ARTICLE
A Simple Procedure for Oral Rehabilitation in a Complex Accident Injury: A Case Report
Reabilitação Oral Simplificada da Sequela Decorrente de Acidente Complexo: Caso Clínico
Luis Carlos da Fontoura Frasca1; Ricardo Smidt2; Aline Montagner3; Elken Gomes Rivaldo4
1Department of Prosthodontics, School of Dentistry, Universidade Federal do Rio Grande do Sul, Porto Alegre, Rio Grande do Sul, Brazil.
2Department of Oral and Maxillofacial Surgery, School of Dentistry, Universidade Luterana do Brasil, Canoas, Rio Grande do Sul, Brazil.
3Graduate Program in Oral and Maxillofacial Surgery, Universidade Luterana do Brasil, Canoas, Rio Grande do Sul, Brazil.
4Department of Prosthodontics, School of Dentistry, Universidade Luterana do Brasil, Canoas, Rio Grande do Sul, Brazil.
ABSTRACT
The use of a removable partial prosthesis is an effective treatment modality in the reconstruction of large maxillary defects, because it provides adequate support for the soft tissue and improves facial contours. Oral functions, such as speech and swallowing, also benefit from the use of removable partial prostheses. Osseointegrated implants are generally not indicated due to systemic factors, lack of bone anchorage, very long treatment times, and high costs. Therefore, the use of a removable partial prosthesis has been proposed as an alternative because of its relatively short treatment time, especially in patients undergoing successive bone- and soft tissue-grafting procedures. This report describes the use of an obturator prosthesis for the prosthetic rehabilitation of a maxillectomy patient with fractures due to a motorcycle accident.
Keywords: Dental prosthesis, wounds and injuries, operative surgical procedures.
RESUMO
O uso de uma prótese parcial removível é uma modalidade de tratamento eficaz na reconstrução de defeitos maxilares grandes, porque fornece um apoio adequado para o tecido mole e melhora o contorno facial. As funções orais como a fala e a deglutição, também se beneficiam com o uso de próteses parciais removíveis. Implantes osseointegrados geralmente não são indicados devido a fatores sistêmicos, deficiência óssea, tempos de tratamento muito longo e custos elevados. Portanto, o uso de uma prótese parcial removível foi proposto como uma alternativa por causa de seu tempo de tratamento relativamente curto, especialmente em pacientes submetidos a sucessivos procedimentos cirúrgicos de enxerto de tecido duro e mole. Este artigo descreve o uso de uma prótese obturadora para a reabilitação protética de um paciente maxilectomizado devido a um acidente de motocicleta.
Palavras-chave: Prótese dentária, ferimentos e lesões, procedimentos cirúrgicos operatórios.
INTRODUCTION
People with facial deformities are often regarded as oral invalids by society. Defects of the oral and maxillofacial region often result from traumatic injuries, surgical tumor resection, and congenital deformities1.
Gunshot injuries and motorcycle accidents are the most common causes of facial fractures. Lacerations followed by neurologic and orthopedic injuries often occur concomitantly with facial fractures2. Facial trauma may result in injuries ranging from mild bruising to severe fractures, leading to irreversible sequelae and sometimes life-threatening complications.
Treatment of trauma patients should start immediately after the accident. Maintenance of upper airway patency, control of bleeding and immobilization are the primary goals, followed by stabilization of vital signs and a neurological examination. Once hospitalized, patients should be resuscitated and constantly monitored, including a more detailed clinical evaluation. Surgical and definitive prosthetic treatments are provided after identification of the lesion, stabilization of the patient, and the results of screening laboratory tests3,4.
Successful treatment of maxillectomy patients requires careful preoperative planning involving a multidisciplinary team: oral and maxillofacial surgeons, oncologists, specialists in speech pathology, prosthodontists, and dental technicians5. Maxillary resection often results in significant bone loss and unpleasant soft tissue morphology, compromising prosthesis retention and stability and creating a direct communication between the oral and nasal cavities6,7. Continuous secretion of mucus in the oral cavity may hinder effective rehabilitation, in addition to leading to dysfunctions in speech and swallowing.
We report the use of a simple and fast procedure for rehabilitation of a patient with fractures in the middle and lower third of the face, with considerable loss of maxillary bone and teeth, due to a motorcycle accident.
CASE REPORT
A 27-year-old Caucasian male motorcyclist crashed into a traffic signal and sustained penetrating facial trauma. The victim reported to be wearing a helmet, but with face shield up, at the time of the crash. The patient was given first aid at the scene of the accident and taken to the emergency department of Hospital de Pronto Socorro de Porto Alegre, southern Brazil, for further evaluation by a multidisciplinary team.
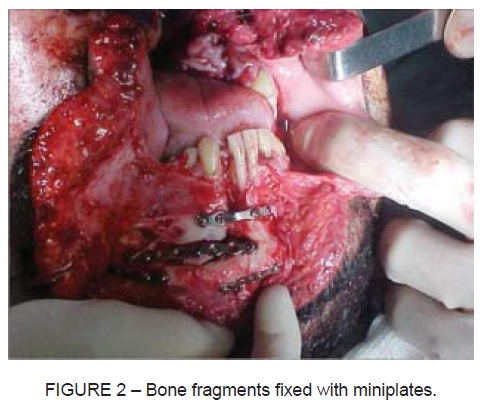
Systemic physical examination revealed no thoracic and/or abdominal injuries. Complex fractures and lacerations of the face were identified (Figure 1). A tracheostomy was performed. The traffic signal acted as a blade, causing a large wound extending from the suprahyoid to the glabellar region. The left side remained intact and the right side was displaced. The patient had a comminuted mandibular fracture, with loss of the mandibular right lateral incisor and anterior lower alveolar process. The left maxillary bone was avulsed and lost in the accident, as well as the maxillary process of the palatine bone. Bone fragments were fixed with miniplates, screws, and stainless steel wire (Figure 2). The vomer bone and inferior nasal turbinates were repositioned and stabilized, as well as the infraorbital arch and zygomatic bone. Vision in the right eye was impaired, without changes in eye movements. All devitalized soft tissue was removed and complete hemostasis was achieved by suture ligation (Figure 3). After 21 days, the patient was discharged home.


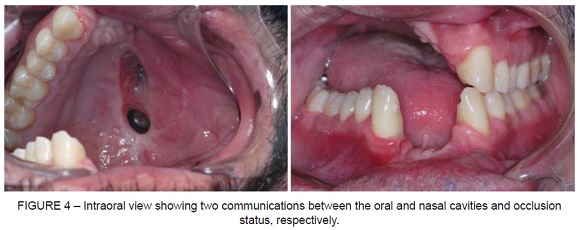
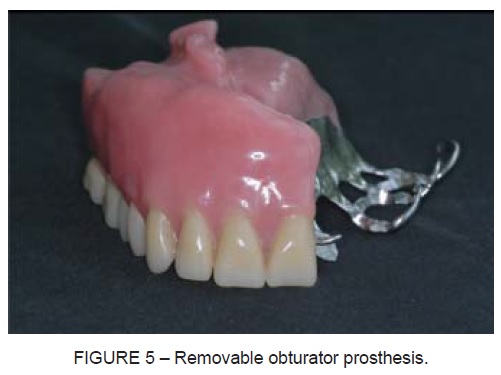
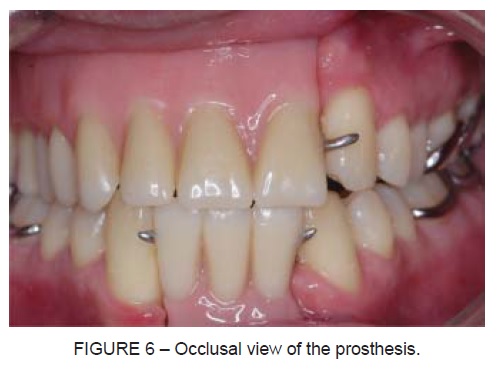
Ninety days after reparative surgery, the patient presented to the School of Dentistry at Universidade Luterana do Brasil, southern Brazil, to treat facial deformities and two communications between the oral and nasal cavities (Figure 4). A removable partial denture obturator was the treatment of choice, supported by residual teeth from the maxillary left canine to the left third molar of the opposite arch (Figure 5). At the same time, a mandibular removable partial prosthesis was placed to ensure stability of mandibular alignment and to replace lost tooth structure. Circumferential clasps and full palatal coverage provided not only adequate retention, bracing and support, but also occlusion of communications between the oral and nasal cavities, reestablishing a support for the lip and bone configurations (Figure 6, Figure 7).

DISCUSSION
Maxillary defects are created by surgical treatment of benign or malignant neoplasms, congenital malformation, and by trauma. The size and location of the defects influence the degree of impairment and difficulty in prosthetic rehabilitation8.
Prosthetic rehabilitation of patients with maxillary resection involving the maxillae, hard and soft palates, and paranasal sinuses represents a significant challenge particularly if the goal is to restore speech, deglutition, mastication, and respiration. Distraction osteogenesis, bone grafts, osseointegrated implants, and magnet attachments may be used to provide retention, support, and stability to a large definitive obturator9. Osseointegrated implants associated with a dental prosthesis have become an effective treatment modality for the replacement of lost structures10. However, although these treatment options have proven effective, lack of bone anchorage and elevated costs have limited their use in this particular case.
A tooth-tissue-supported removable prosthesis was an excellent alternative to replace all lost structures in this case11. The patient had a sufficient number of teeth and their position was considered appropriate to provide adequate retention and stability.
In conclusion, a tooth-tissue-supported removable partial prosthesis was fabricated for this patient due to systemic, financial, and osseous limitations. This simple treatment was effective in restoring mastication and improving speech, deglutition and the aesthetic outcome without further surgery, thus significantly increasing the patient’s quality of life.
REFERENCES
1. Omondi BI, Guthua SW, Awange DO, Odhiambo WA. Maxillary obturator prosthesis rehabilitation following maxillectomy for ameloblastoma: case series of five patients. Int J Prosthodont 2004;17:464-8. [ Links ]
2. Haug RH, Prather J, Indresano AT. An epidemiologic survey of facial fractures and concomitant injuries. J Oral Maxillofac Surg 1990;48:926-32. [ Links ]
3. Ali J, Adam R, Butler AK, Chang H, Howard M, Gonsalves D, Pitt-Miller P, Stedman M, Winn J, Williams JI. Trauma outcome improves following the advanced trauma life support program in a developing country. J Trauma 1993;34:890-8. [ Links ]
4. Fonseca RJ, Walker RV, Betts NJ. Oral and Maxillofacial Trauma, 2th ed. New York: Elservier;1997. p.3-243. [ Links ]
5. Dexter WS, Jacob RF. Prosthetic rehabilitation after maxillectomy and temporalis flap reconstruction: a clinical report. J Prosthet Dent 2000;83:283-6. [ Links ]
6. Desjardins RP. Obturator prosthesis design for acquired maxillary defects. J Prosthet Dent 1978;39:424-35. [ Links ]
7. Curtis TA, Beumer J. Restoration of acquired hard palate defects: etiology, disability and rehabilitation: In: Beumer J, Curtis TA, Marunick MT. Maxillofacial rehabilitation: prosthodontic and surgical considerations. St. Louis: Ishiyaku EuroAmerica; 1996. p.225-84. [ Links ]
8. Keyf F. Obturator prostheses for hemimaxillectomy patients. J Oral Rehabil. 2001 Sep; 28(9): 821-9. [ Links ]
9. Oh WF, Roumanas E. Dental implant-assisted prosthetic rehabilitation of a patient with a bilateral maxillectomy defect secondary to mucormycosis. J Prosthet Dent. 2006 Aug; 96(2): 88-95. [ Links ]
10. Kreissl ME, Heydecke G, Metzger MC, Schoen R. Zygoma implant-supported prosthetic rehabilitation after partial maxillectomy using surgical navigation: a clinical report. J Prosthet Dent. 2007 Mar; 97(3): 121-8. [ Links ]
11. Pigno MA. Conventional prosthetic rehabilitation after free flap reconstruction of a maxillectomy defect: a clinical report. J Prosthet Dent 2001;86:578-81. [ Links ]
 Corresponding Author:
Corresponding Author:
Luis Carlos da Fontoura Frasca
Av. Vinte e quatro de outubro, 1439, Bairro Auxiliadora
CEP 90510–003 – Porto Alegre, RS – Brazil
Telephone/fax: +55 51 99829802
E-mail:lcfrasca@terra.com.br
