










Services on Demand
Article
 pdf in English
pdf in English Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailRelated links
Share

 Permalink
PermalinkRGO.Revista Gaúcha de Odontologia (Online)
On-line version ISSN 1981-8637
RGO, Rev. gaúch. odontol. (Online) vol.61 n.1 Porto Alegre Jan./Mar. 2013
ORIGINAL / ORIGINAL
Effectiveness of manual and electric brushes in the removal of biofilm from full dentures
Eficácia das escovas manual e elétrica na remoção do biofilme de próteses totais
Ingrid Machado de ANDRADEI; Patrícia Costa CRUZI; Bárbara Fuzaro ZAMBONEI; Cláudia Helena SILVA-LOVATOI; Raphael Freitas de SOUZAI; Maria Cristina Monteiro de SOUZA-GUGELMINII; Helena de Freitas Oliveira PARANHOSI
I Universidade de São Paulo, Faculdade de Odontologia, Departamento de Materiais Dentários e Prótese
II Universidade de São Paulo, Faculdade de Ciências Farmacêuticas, Departamento de Análises Clínicas, Toxicológicas e Bromatológicas. Ribeirão Preto, SP, Brasil
ABSTRACT
Objective
To evaluate clinically the ability to remove biofilm from complete dentures.
Methods
Thirty patients, users of full upper dentures, participated in a trial period of 21 days and were instructed to brush the dentures three times a day (after breakfast, lunch and dinner) with water, using a manual, special denture brush (Group I - Control) and electric brush (Group II - Experimental). At night, the patients were instructed to immerse their dentures in a container with filtered water. Before and after the use of these methods for 21 days, the internal surfaces of the complete upper dentures were stained (1% neutral red) and photographed. The areas (total of internal surface and the surface stained with biofilm) were quantified using software (Image Tool 2.02). The percentage of the biofilm was calculated as the ratio of the area of the biofilm multiplied by 100 to the total surface area of the internal base of the dentures.
Results
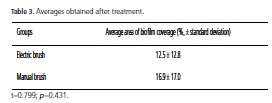
The data for the two methods were compared using the Student's t-test (αα = 0.05). There was a mean area of biofilm coverage (%, ± standard deviation) of 12.5 ± 12.8 and 16.9 ± 17.0 for the manual and electric toothbrushes, respectively. The differences were not significant (t = 0.799, P = 0.431).
Conclusion
It was concluded that both brushes tested showed the same capacity for biofilm removal from complete dentures.
Indexing terms: Biofilm. Denture cleansers. Denture complete. Tooth brushing.
RESUMO
Objetivo
Avaliar clinicamente a capacidade de remoção do biofilme de prótese total de dois métodos mecânicos de higiene: escovação manual e elétrica.
Métodos
Trinta pacientes, usuários de próteses totais superiores, participaram de um período experimental de 21 dias e foram orientados a escovar as próteses três vezes ao dia (após café da manhã, almoço e jantar) com água empregando escova manual específica para próteses totais (Grupo I - Controle) e elétrica (Grupo II - Experimental). Durante o período noturno o paciente foi orientado a imergir suas próteses em recipiente contendo água filtrada. Antes e após o uso dos métodos por 21 dias, as superfícies internas das próteses totais superiores foram evidenciadas (vermelho neutro 1%) e fotografadas. As áreas (total da superfície interna e corada com biofilme) foram quantificadas com um software (Image Tool 2.02). A porcentagem do biofilme foi calculada como a relação entre a área do biofilme multiplicado por 100 e a área da superfície total da base interna da prótese.
Resultados
Os dados dos dois métodos foram comparados por meio do teste t de Student (αα = 0,05). Observou-se uma área média de cobertura por biofilme (%, ±desvio padrão) de 12,5±12,8 e 16,9±17,0 para a escova elétrica e a manual, respectivamente. As diferenças não foram significantes (t=0,799; p=0,431).
Conclusão
Concluiu-se que ambas as escovas testadas apresentaram a mesma capacidade de remoção de biofilme das próteses totais.
Termos de indexação: Biofilmes. Higienizadores de dentadura. Prótese total. Escovação dentária.
INTRODUCTION
The oral health of elderly individuals who use complete or partial dentures can be precarious1-2, it being common for lesions associated with trauma and deficient hygiene to arise3-4. These aspects point to a need to educate the denture user insofar as caring for functional maintenance of the prosthetic appliance and the health of oral tissue is concerned. Therefore, the removal of biofilm by means of proper cleaning is of the utmost importance to the oral health of the complete denture user.
Biofilm is defined as a dense microbial layer formed by microorganisms and their metabolites5. Correct removal of biofilm results in reduced accumulation of organic material and proliferation of bacteria and fungi that could cause malodour6, pigmentation and staining of the acrylic resin, formation of calculus and development of Chronic Atrophic Candidiasis7. In some cases the
spreading of microorganisms and the appearance of lung or gastrointestinal infections may occur8-9.
Two methods are proposed to this end: mechanical and chemical. The mechanical methods are classified as brushing (with water, soap, paste or abrasives) and ultrasonic devices. The chemical methods are classified as hypochlorites, peroxides, neutral peroxides with enzymes, enzymes, acids, crude drugs and mouthrinses8.
There is still no consensus over which method is the most efficient for oral and denture hygiene, as studies have demonstrated contradictory results with regard to these methods; in some cases the chemical method is superior, in other the mechanical method is better and in some cases there is little to choose between them in terms of effectiveness. Netto et al.10 studied the effect of chlorhexidine, stannic fluoride and instructed brushing on the formation of dental biofilm and they observed that there was no statistical difference between the three
methods.
Of all the methods, brushing is the most wellknown and has the advantage of being simple, inexpensive and effective11-12, however it presents difficulties for patients with poor motor coordination and produces roughness on the surface of the acrylic resin13. In this way, it is essential to use brushes and the appropriate auxiliary agents. According to Naressi & Moreira14, to prevent the buildup of biofilm and the spread of infections in patients, it is of the utmost importance that the professional supplies the patient with the proper brush and asks him to try and remove the biofilm, using his usual brushing technique and that he then shows him the various areas that failed to be cleaned properly, providing guidance on the most appropriate way to carry out the brushing.
It should be stressed that electric brushes can also be acquired on the market. Brushing with an electric brush has been put forward as an option, mainly for patients with motor and cognitive difficulties15. Electric brushes produce fewer grooves on the surface of the dentures, as the force exerted by the patient is minimal16. However, the cost of these brushes is higher than for
manual brushes.
In a clinical evaluation of elderly patients with lower implant-mucosa-supported dentures, Tawse-Smith et al.17 observed that electric and manual brushes were equally efficient in controlling supragingival biofilm and tissue inflammation.
On the other hand, Heasman et al.16, comparing the effectiveness of two electric brushes with one manual brush, in 75 young patients, noted that after six weeks of treatment, the electric brush group presented a lower quantity of biofilm than the manual brushing group, but the differences were only significant on the proximal surfaces.
Electric brushes have been recommended as important auxiliary agents in controlling the biofilm in patients with teeth18-20; however studies related to the use of these products by complete denture wearers have not been reported. Accordingly, the aim of the present study was to evaluate the effectiveness of the use of electric brushes in respect of the property of removing biofilm from complete dentures, and comparing them with manual brushes.
METHODS
After the approval of the research project by the Ethics Committee at the Ribeirão Preto Faculty of Dentistry (USP) (Filing no. 2003.1.1369.58.4), and the signing of a patient consent form, 30 patients were selected from the Full Prosthesis clinic, of both sexes, aged between 48 and 84 (average age of 64), with a good overall state of health and users of full upper dentures made from thermally polymerized acrylic resin, without cracks or patches and having used the denture for at least 5 years. As for the presence of biofilm, the dentures were selected according to the Ambjørnsen Additive Index21, and only subjects wearing upper complete dentures with scores of "1" or higher were selected.
Distribution of patients into groups
The patients were randomly allocated to two groups: a) control group: denture brushing using a brush that is specific for complete dentures (Bitufo - Valinhos, Brazil) and water; b) experimental group: brushing of the dentures with an electric brush (Oral B - Oral B Serviço, Indústria e Comércio Ltda., São Paulo, Brazil) and water.
To clean the dentures, the patients were instructed to brush all surfaces of the complete dentures for 2 minutes, 3 times a day, after meals (breakfast, lunch and dinner), with the supplied brushes, to rinse the oral cavity with tap water and after each brushing of the dentures, immerse the dentures in water overnight.
By means of a practical demonstration of brushing, both groups received instruction, observing the following criteria: Moistening of the bristles with water, holding the dentures in the palm of the hand over a sink containing water to avoid damage to the prosthetic appliance in the event that the denture is dropped during brushing; brushing of the (internal and external) surfaces of the dentures for 2 minutes.
The products were used for 3 consecutive weeks, i.e. the experiment lasted 21 days.
Disclosure biofilm
Initially, the biofilm that was present on the internal surface was totally removed through professional cleaning with a brush specific to complete dentures, (Denture - Condor S.A., São Bento do Sul, Brazil) and liquid soap (Fennel Liquid Soap - JOB Química Produtos para Limpeza Ltda., Ribeirão Preto, Brazil). After 21 days using the products, disclosure procedure was carried out using neutral red solution at 1% and a photograph was taken of the biofilm buildup on the internal surface of the complete upper dentures. The digital camera (Nikon, Coolpix 950) was positioned on the stand with the lens turned towards the internal surface of the denture at an angle of 45o. The distance was determined by the focus of the central region of the palate of the largest denture. Then the stained dentures were cleaned once again by the professional, using a specific brush (Denture) and liquid soap (JOB Química Produtos para Limpeza Ltda., Ribeirão Preto, Brazil) and returned to the patients.
Biofilm quantification
The contours of the total area of the denture and the area with biofilm, needed to determine the percentage of biofilm buildup on the denture, were marked on t h e Image Tool, (Windows version 3.0, The University of Texas Health Science Center). Once the measurements of the two areas (total and biofilm) were completed, the percentage of the surface covered in biofilm was calculated as being the ratio of the area of biofilm multiplied by 100 to the total surface area of the internal base of the denture. The data from the two methods were compared by way of the Student's t-test (p < 0.05).
RESULTS
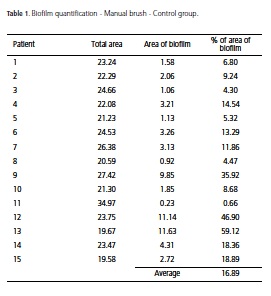
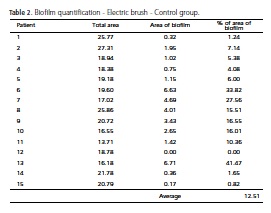
Employing the Image Tool quantitative method, the initial results for the areas (total and biofilm) of the internal surfaces of the full upper dentures, after 21 days using these treatments, are shown in Tables 1 and 2.
For both groups, the majority of patients (n=12; 80%) had up to 20% of the analyzed area covered by biofilm. In the manual brushing group, only one patient (6.7%) presented 50% of the total area of the denture covered in biofilm. In the group with the electric brushes, three patients (20%) exhibited biofilm percentages between 20% and 50%; and just one patient (6.7%) presented no biofilm on the denture surface. It was noted that the percentage averages of the areas of biofilm for the two evaluated groups, i.e. the manual brushing group and the group with the electric brushes, were 16.9% and 12.5%, respectively.
Statistical analysis
The data in the two methods were compared by means of the Student's t-test (αα= 0.05). The software application SPSS, version 12.0.0 for Windows (SPSS Inc., Chicago, Ill, USA) was used for the analysis. An average area of biofilm coverage was observed (%, ± standard deviation) of 12.5 ± 12.8 and 16.9 ± 17.0 for the electric brush and manual brush, respectively (Table 3). The differences were not significant (t=0.799; p=0.431).
DISCUSSION
One of the measures of effectiveness of a complete denture cleaning agent is its ability to remove biofilm. Nikawa et al.8 call attention to the need for this effectiveness to be evaluated through clinical studies as in vitro results are not always in agreement with clinical reality.
In the present study, the effectiveness of the products was evaluated for the internal surfaces of full upper dentures, as this represents an area of large buildup of biofilm and great clinical importance in terms of the relationship to pathologies found in complete denture wearers. The analysis of the external surfaces was not included, as it represents an area that is far easier to clean, with lower levels of biofilm than the corresponding internal surface22-23.
Studies report greater efficiency with the electric brush versus the manual brush, principally as far as the removal of biofilm is concerned24-25, while other works have reported that the electric brush possesses no advantage over the manual brush26. There are no studies in the literature, however, that have evaluated the efficiency of the electric brush in removing prosthetic biofilm. The majority of studies on electric brushes deal with the removal of biofilm in patients that have teeth, principally in the periodontal and pediatric areas. Accordingly, the present study sought to evaluate clinically the effectiveness of manual and electric brushing in terms of the properties of biofilm removal of complete dentures.
In the present study, the statistical analysis employed (Student's t-test) showed there was no significant difference between manual and electric brushing. Both were effective in reducing biofilm when patients brushed three times a day for 21 days, using only water.
The results presented here are in agreement with the study by Moran et al.27 who compared the effectiveness of an electric brush with a manual brush with the removal of chlorhexidine/tea stains from teeth. The authors concluded that both brushes removed a large part of the stains in just one brushing session and that the cleaning effectiveness of the two types of brush was statistically similar.
In a parallel study, van der Weijden et al.28 noted, on comparing the effect of electrical and manual brushes in removing biofilm and gingivitis in a seven-month clinical trial, that no improvement was observed after using the manual brush, bearing in mind that an increase in bleeding was observed in the test group during the course of the study. They concluded that no difference was observed between the brushes during the test period of seven months.
It should be stressed, however, that the results obtained here contradict those observed by Carter et al.29, who concluded that the electric brush may be safely used and that it promotes additional benefits over the manual brush in the reduction of the rates of calculus and also the incidence of biofilm. However, contrary to the present study, usage instructions were not given for each type of brush and perhaps the differences in the outcome reflect this fact.
The results found by Lazarescu et al.30, who compared the effectiveness of removing biofilm from electric and manual brushes in the general population and analyzed the effect of giving instruction on proper usage, are also in opposition. The authors observed that, after 18 weeks, the biofilm index dropped significantly in the significantly more effective in removing biofilm and improving gingival health in the group of patients not familiar with electrical brushes. It is important to emphasize that, in the methodology used in this study, a dentrifice was used for the brushing, which could have produced the discrepancy in the outcome, in contrast with the present study.
Similarly, Heasman et al.16 concluded in their study that electric brushes are more effective than manual brushes in removing biofilm although a statistically significant difference was only found with the interproximal surfaces. However, unlike in the present study, a dentrifice was used in conjunction with the brushes, which could have resulted in the difference in the efficiency between the two types of brushes.
It should be stressed that, in the present study, there were two limitations: the first limitation relates to the reduced sample, explained by the difficulty in selecting complete denture wearers who came within the criteria demanded by the study in question; the second involves the low levels of biofilm found after the use of the manual and electric brushes, which may be explained by the knowledge acquired by the patients in an earlier study on proper brushing.
So, for future studies, it is proposed to study a more representative sample of complete denture wearers and a group that has not received instructions on how to brush, so as to ascertain the true effectiveness of the manual and electric brushes when the patient carries out his/her daily brushing. It is also planned to test the antimicrobial action after the use of the manual and electric brushes and ascertain if the electric brush could be recommended as the standard for the cleaning of complete dentures.
CONCLUSION
Given the limitations of this study, it was possible to conclude that both methods (manual and electrical brushing) were equally effective in terms of the removal of biofilm from complete dentures, and they may be used as auxiliary agents in maintaining the oral hygiene of complete denture wearers.
Acknowledgements
The present study was carried out with the backing of FAPESP, the São Paulo Research Foundation (no. 2005/55705-2).
Collaborators
IM ANDRADE and PC CRUZ took part in the performance of the experimental work in the clinic, the organization and distribution of the materials, guidance to patients and were responsible for coordinating the return visits as well as the composition of the article. BF ZAMBONE was responsible for measuring the biofilm by means of a reading of photographs using the image tool, and the composition of the article. CH Silva-Lovato took part in the performance of the experimental work in the clinic, the distribution of materials, guidance for patients and was responsible for taking the photographs and the composition of the article. RF SOUZA was responsible for the statistical analysis and interpretation, took part in the performance of the experimental work and the composition of the article. MCM SOUZA-GUGELMIN jointly directed the study and took part in the performance of the experimental work and the composition of the article. HFO PARANHOS directed the work and participated in organizing the planning of the experiments, the performance of the experimental work in the clinic and the composition of the article.
REFERENCES
1. Kanli A, Demirel F, Sezgin Y. Oral candidosis, denture cleanliness and hygiene habits in an elderly population. Aging Clin Exp Res. 2005;17(6):502-7. [ Links ]
2. Marchini L, Vieira PC, Bossan TP, Montenegro FL, Cunha VP. Self-reported oral hygiene habits among institutionalized elderly and their relationship to the condition of oral tissues in Taubate,
Brazil. Gerodontology. 2006;23(1):33-7. doi: 10.1111/j.1741-2358.2006.00092.x.
3. Coelho CM, Souza YT, Dare AM. Denture-related oral mucosal lesions in a Brazilian school of dentistry. J Oral Rehabil. 2004;31(2):135-9. doi: 10.1111/j.1365-2842.2004.01115.x. [ Links ]
4. Marchini L, Tamashiro E, Nascimento DFF, Cunha VP. Selfreported denture hygiene of a sample of edentulous attendees at a University dental clinic and the relationship to the condition of the oral tissues. Gerodontology. 2004;21(4):226-8. doi: 10.1111/j.1741-2358.2004.00026.x. [ Links ]
5. Nikawa H, Hamada T, Yamamoto T. Denture plaque–past and recent concerns. J Dent. 1998;26(4):299-304. doi: 10.1016/ S0300-5712(97)00026-2.
6. Verran J. Malodour in denture wearers: an ill-defined problem. Oral Dis. 2005;11(suppl. 1):24-8. [ Links ]
7. Akpan A, Morgan R. Oral candidiasis. Postgrad Med J. 2002;78(1):455-9. doi: 10.1136/pmj.78.922.455. [ Links ]
8. Nikawa H, Hamada T, Yamashiro H, Kumagai H. A review of in vitro and in vivo methods to evaluate the efficacy of denture cleansers. Int J Prosthodont. 1999;12(2):153-9. [ Links ]
9. Imsand M, Janssens JP, Auckenthaler R, Mojon P, Budtz-Jørgensen E. Bronchopneumonia and oral health in hospitalized older patients: a pilot study. Gerodontology. 2002;19(2):66-72. doi: 10.1111/j.1741-2358.2002.00066.x. [ Links ]
10. Netto RL, Macedo NL, Lima FR, Souza WLA, Ferreira UR. Efeito da escovação orientada, do fluoreto estanhoso e da clorexidina sobre a formação da placa bacteriana. RGO - Rev Gaúcha Odontol. 1987;35(4):259-63. [ Links ]
11. Paranhos HFO, Silva-Lovato CH, Souza RF, Cruz PC, Freitas KM, Peracini A. Effects of mechanical and chemical methods on denture biofilm accumulation. J Oral Rehabil. 2007;34(8):606- 12. doi: 10.1111/j.1365-2842.2007.01753.x. [ Links ]
12. Paranhos HFO, Silva-Lovato CH, Venezian GC, Macedo LD, Souza RF. Distribution of biofilm on internal and external surfaces of upper complete dentures: the effect of hygiene instruction.
Gerodontology. 2007;24(3):162-8. doi: 10.1111/j.1741-2358.2007.00177.x.
13. Harrison Z, Johnson A, Douglas CW. An in vitro study into the effect of a limited range of denture cleaners on surface roughness and removal of Candida albicans from conventional heat-cured acrylic resin denture base material. J Oral Rehabil. 2004;31(5):460-7. doi: 10.1111/j.1365-2842.2004.01250.x. [ Links ]
14. Naressi WG, Moreira EJG. Odontologia preventiva. RGO - Rev Gaúcha Odontol. 1983;31(3):281-3. [ Links ]
15. Ciancio S. Electric toothbrushes - for whom are they designed? Adv Dent Res. 2002;16(1):6-8. doi: 10.1177/154407370201600103. [ Links ]
16. Heasman PA, Stacey F, Heasman L, Sellers P, Macgregor IDM, Kelly PJ. A comparative study of the Philips HP 735, Braun/Oral B D7 and the Oral B 35 Advantage toothbrushes. J Clin Periodontol. 1999;26(2):85-90. doi: 10.1034/j.1600-051X.1999.260204.x. [ Links ]
17. Tawse-Smith A, Duncan WJ, Payne AG, Thomson WM, Wennstrom JL. Relative effectiveness of powered and manual toothbrushes in elderly patients with implant-supported mandibular overdentures. J Clin Periodontol. 2002;29(4):275-80. doi: 10.1034/j.1600-051X.2002.290401.x. [ Links ]
18. Cronin MJ, Dembling WZ, Cugini MA, Thompson MC, Warren PR. Three-month assessment of safety and efficacy of two electric toothbrushes. J Dent. 2005;33(Suppl 1):23-8. doi:
10.1016/S0300-5712(05)80004-1.
19. Goyal CR, Sharma NC, Oagish JG, Cugini MA, Thompson MC, Warren PR. Efficacy of a novel brush head in the comparison of two power toothbrushes on removal of plaque and naturally occurring extrinsic stain. J Dent. 2005;33(Suppl. 1):37-43. doi: 10.1016/S0300-5712(05)80006-5. [ Links ]
20. Sharma NC, Oagish JG, Galustians HJ, Goyal CR, Cugini MA, Thompson MC, et al. Plaque removal efficacy of two electric toothbrushes with different brush head designs. J Dent. 2005;33(Suppl. 1):17-21. [ Links ]
21. Ambjørgensen E, Vauderhaug J, Norheim PW, Fløystrand F. Assessment of an additive index for plaque accumulation on complete maxillary dentures. Acta Odontol Scand. 1982;40(4):203-8. [ Links ]
22. Fernandes RAG, Silva-Lovato CH, Paranhos HFO, Ito IY. Eficácia de escovas para próteses totais: propriedade de remoção de biofilme e ação antimicrobiana. Braz Oral Res. 2006;20(1):252. [ Links ]
23. Paranhos HFO, Lara EHG, Panzeri H, Candido RC, Ito IY. Capacity of denture plaque/biofilm removal and antimicrobial action of a new denture paste. Braz Dent J. 2000;11(2):97-104. [ Links ]
24. van der Weijden GA, Timmerman MF, Reijerse E, Snoek CM, van der Velden U. Comparison of two electric toothbrushes in plaque removing ability. Professional and supervised brushing. J Clin Periodontol. 1995;22(8):648-52. doi: 10.1111/j.1600-051X.1995.tb00819.x [ Links ]
25. Quirynen M, Vervliet E, Teerlinck J, Darius P, van Steenberghe D. Medium - and long-term effectiveness of a counter-rotational electric toothbrush on plaque removal, gingival bleeding, and probing pocket depth. Int J Periodontics Restorative Dent. 1994;14(1):364-77. [ Links ]
26. Ainamo J, Hormia M, Kaunisaho K, Sorsa T, Suomalainen K. Effect of manual versus powered toothbrushes. J Dent Res. 1991;70(1):557. [ Links ]
27. Moran J, Addy M, Courtney M, Smith S, Newcombe R. A clinical study to assess the ability of a powered toothbrush to remove chlorhexidine/tea dental stain. J Clin Periodontol. 2004;31(1):95-8. doi: 10.1111/j.0303-6979.2004.00449.x. [ Links ]
28. van der Weijden GA, Timmerman MF, Piscaer M, Snoek I, van der Velden U, Galgut PN. Effectiveness of an electrically active brush in the removal of overnight plaque and treatment of gingivitis.
J Clin Periodontol. 2002;29(1):699-704. doi: 10.1034/j.1600-051X.2002.290806.x.
29. Carter K, Landini G, Walmsley AD. Plaque removal characteristics of electric toothbrushes using an in vitro plaque model. J Clin Periodontol. 2001;28(11):1045-9. doi: 10.1111/j.1600-
051X.2001.281109.x.
30. Lazarescu D, Boccaneala S, Iliescu A, De Boever JA. Efficacy of plaque removal and learning effect of a powered and a manual toothbrush. J Clin Periodontol. 2003;30(8):726-31. doi:
10.1034/j.1600-051X.2003.00361.x.
 Correspondence to:
Correspondence to:
IM ANDRADE
Av. do Café, s/n., Monte Alegre, 14040-904, Ribeirão Preto, SP, Brasil.
e-mail: ingridma76@yahoo.com.br
Received on: 10/6/2009
Final version resubmitted on: 21/10/2009
Approved on: 10/11/2009
