










Services on Demand
Article
 pdf in English
pdf in English Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailRelated links
Share

 Permalink
PermalinkRSBO (Online)
On-line version ISSN 1984-5685
RSBO (Online) vol.8 n.4 Joinville Oct./Dec. 2011
ORIGINAL RESEARCH ARTICLE
Comparison of canal transportation and centering ability of hand Protaper files and rotary Protaper files by using micro computed tomography
Amit GandhiI; Taru GandhiII
I MDS, Reader, Department of Conservative Dentistry and Endodontics, Prabhu Dayal Memorial Dental College and Research Institute – Bahadurgarh – Haryana – India
II BDS, Private Practice, Gandhi Dental Clinic – Rohtak – Haryana – India
ABSTRACT
Introduction and objective: The aim of the present study was to compare root canal preparation with rotary ProTaper files and hand ProTaper files to find a better instrumentation technique for maintaining root canal geometry with the aid of computed tomography. Material and methods: Twenty curved root canals with at least 10 degree of curvature were divided into 2 groups of 10 teeth each. In group I the canals were prepared with hand ProTaper files and in group II the canals were prepared with rotary ProTaper files. Image analysis was performed at four levels 4mm, 6mm, 9mm, and 12mm from the root apex to assess changes in canal transportation and centering ratio using computed tomography (CT). Results: Data suggest that rotary ProTaper files presented the best outcomes for both variables evaluated. Rotary ProTaper files caused lesser transportation and remained better centered in the canal than hand ProTaper files. Conclusion: The canal preparation in natural teeth with rotary Protaper files showed lesser transportation and better centering ration than hand ProTaper files.
Keywords: canal shaping; centering ratio; computed tomography; transportation.
Introduction
The cleaning and shaping of root canal space is one of the most important and fundamental aspects of endodontic therapy. The literature is replete with articles describing that shaping procedures can produce aberrations such as zips, elbows, danger zones, perforations and ledges which compromise the integrity of the root itself and lead to difficulties in obturation.
Civjan (1975) was one of the first investigators to propose nickel-titanium alloy for use in Endodontics 1. According to Walia et al. (1988), the advent of nickel-titanium instruments not only provided greater flexibility but also raised the possibility of automated instrumentation which could conceivably reduce the need for highly developed tactile skills and bring advanced endodontic practice in use 12.
Although hand files made of Ni-Ti are available, engine driven rotary techniques and instruments have revolutionized root canal preparation and are gaining in popularity. ProTaper instruments show a convex triangular cross-sectional design with an advanced flute design that combines multiple taper within the shaft. This feature claims to reduce the contact area between file and dentine. Nevertheless, this feature predisposes the canal to greater transportation.
Tachibana and Matsumoto evaluated the applicability of computed tomography (CT) in Endodontics in 1989. Canal preparation performed by Ni-Ti and stainless steel hand instruments on simulated canals 2,3 and extracted teeth 5,10 have been compared using CT. CT provides a non-invasive and three dimensional view inside canal system of teeth. It is possible to scan teeth before and after instrumentation, and than compare the before and after images of canal systems. The aim of the present study was to compare the root canal preparation with rotary ProTaper files and hand ProTaper files to find a superior instrumentation technique for maintaining root canal geometry with the aid of computed tomography.
Material and methods
Specimen selection and preparation
The present study was carried out in vitro on 20 intact permanent freshly extracted human single rooted teeth with at least 10 degree of curvature at mesial-distal plane. The collected teeth were thoroughly washed and cleaned of all debris/calculus. They were stored in 10% formalin. The crowns of all the specimens were sectioned 17 mm short from the apex.
Access cavities were prepared by using a #4 high speed round carbide bur (Dentsply, Maillefer). A size 10 K-flexofile (Dentsply, Maillefer) was placed into the canal until it was visible at the apical foramen, and working length (WL) was established 0.5 mm short of this length. Teeth were then radiographed from bucco-lingual aspect. The radiographs were then scanned. The images so recorded were taken into vector drawing and edited using Coral Draw 9.0 software and an outline in vector form was drawn around the tooth and also the root canal. Canal curvature was calculated by the method describe by Schneider 9. Twenty two teeth with at least 10 degree of curvature at mesial-distal plane were selected.
Scanning and imaging of uninstrumented teeth
Twenty teeth were divided into two groups of 10 teeth each (group I and group II). Specimens were then partially embedded into transparent acrylic; the teeth were placed in order that all were aligned in same direction. The specimens were placed into CT Unit (General Electric, Milwaukee, WI) and aligned so that the long axis of the roots was perpendicular to the beam. The teeth were then scanned to determine root canal shape at 4 mm, 6 mm, 9 mm, and 12 mm from root apex.
Canal instrumentation
After the initial scans, the specimens were removed from the acrylic block, and were instrumented. In group I, the canals were instrumented with hand ProTaper files (Dentsply, Maillefer) using crown down technique according to manufacturers recommendations. The shaping procedure commenced with #15 K-file to full WL, then S-X to two-third of length, followed by S1 and S2 to full WL. Shaping continued with F1 finishing instrument followed by F2, F3 to WL. In Group II, the canals were instrumented with rotary ProTaper files (Dentsply, Maillefer) using 128:1 reduction geared hand piece powered by electric motor (Anthogyr, France) according to manufacturer's recommendations. The procedure was the same as described for hand Protaper files.
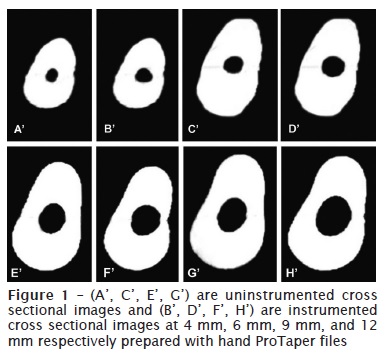
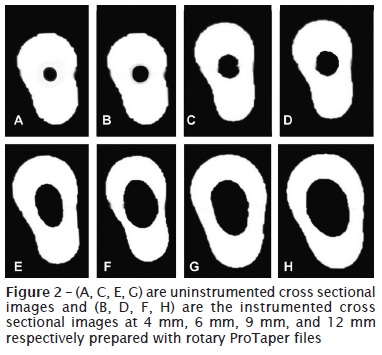
Through the entire sequence of operation, recapitulation using ISO #10K file and irrigation with 2.5% sodium hypochlorite was done after every instrument. Glyde (Dentsply, Maillefer) was used as a lubricant during instrumentation. After instrumentation, the teeth were returned to the acrylic blocks and repositioned in the same orientation use for the first scan. The specimens were again scanned exactly as described for the uninstrumented specimens. Data were stored on a magnetic optical disc (figures 1, 2).
Evaluation of canal transportation
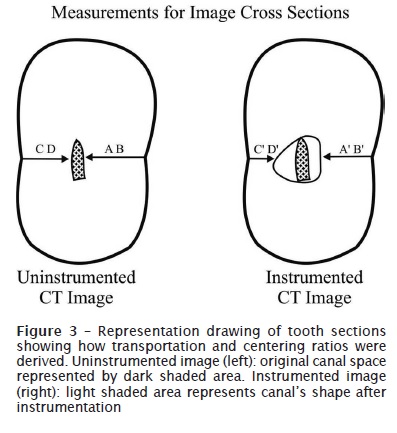
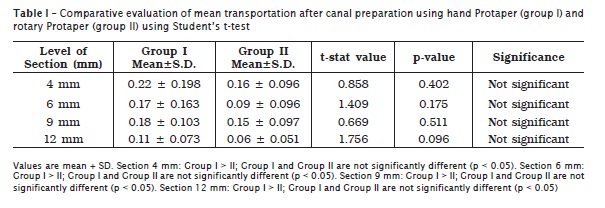
The following formula was used for calculation of canal transportation: [(CD-C'D')-(AB-A'B')], where CD represented the shortest distance from the outside of the curved root to the periphery of the uninstrumented canal. C'D' represented the shortest distance from the outside of the curved 377root to the periphery of the instrumented canal. AB represented the shortest distance from the inside of the curved root to the periphery of the uninstrumented canal. A'B' represented the shortest distance from the inside of the curved root to the periphery of the instrumented canal (figure 3). According to this formula, a result other than 0 indicates that transportation has occurred in the canal. Student's t-test was used for comparative evaluation of mean transportation after canal preparation using hand ProTaper (group I) and rotary ProTaper (group II).
Evaluation of centering ability
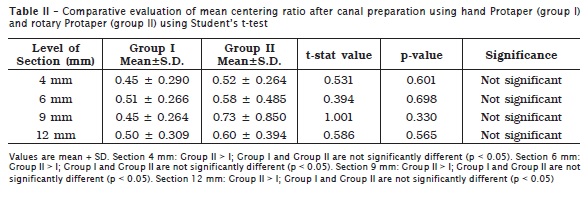
The mean centering ratio indicates the ability of the instrument to stay centered in the canal. This ratio was calculated for each section using the following ratio:
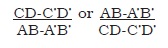
If these numbers are not equal, the lower figure is considered as the numerator of the ratio. According to this formula, a result of 1 indicates perfect centering. Student's t-test was used for comparative evaluation of mean centric ratio after canal preparation using hand ProTaper (group I) and rotary ProTaper (group II).
Results
Canal transportation
The mean transportation for group I at 4 mm, 6 mm, 9 mm and 12 mm sections were 0.22 mm, 0.17 mm, 0.18 mm, and 0.11mm, respectively. The mean transportation for group II at 4 mm, 6 mm, 9 mm and 12 mm sections were 0.16 mm, 0.09 mm, 0.15 mm and 0.06 mm, respectively. Statistical analysis showed a t-value at 4 mm, 6 mm, 9 mm and 12 mm sections for group I and II of 0.858, 1.409, 0.669, and 1.756, respectively (table I). These results showed there was no significant difference between the groups (P > 0.05).
Centering ratio
The mean centering ratio for group I at 4 mm, 6 mm, 9 mm, and 12 mm sections were 0.45, 0.51, 0.45, and 0.50, respectively. The mean centering ratio for group II at 4 mm, 6 mm, 9 mm, and 12 mm sections were 0.52, 0.58, 0.73, and 0.60, respectively. Statistical analysis showed a t-value at 4 mm, 6 mm, 9 mm and 12 mm sections for group I and II of 0.531, 0.394, 1.001, and 0.586, respectively (table II). These results showed that there was no significant difference between the groups (p > 0.05).
Discussion
The cleaning and shaping of the root canal space is one of the most important and fundamental aspects of endodontic therapy. The present study was an attempt to evaluate and compare the shaping ability of hand ProTaper files (group I), and rotary ProTaper files (group II) in root canal preparation.
The ProTaper files are used in crown-down technique to avoid stress on instruments by early opening of the coronal part of the root canal. In their study Morgan and Montgomery (1984) suggested that crown down technique received more significantly excellent ratings than the step back method with almost similar occurrence of zipping and questionable occurrence of ledging and perforation in either technique 6. The apical area of all root canals were prepared to F3, as it has been shown that apical preparations to larger size instruments facilitates proper irrigation and better obturation with gutta-percha 11.
Extracted teeth were used in this in vitro study to assess instrumentation of curved canals. Although resin canals as substitutes for canals in extracted roots can also be used, they have not been considered ideal to be used for the study of rotary instruments because they are not cut in the same way as dentine owing to the difference in micro-hardness between dentine (35 to 40 kg/mm2) and resin (20 to 22 kg/mm2). Moreover heat generated by rotary motion can soften the resin.
Overall, in all 4 sections rotary ProTaper files showed less canal transportation (table I) and better centering ability (table II) than hand ProTaper files but the results were not statistically significant between the two groups. The study conducted by Ottosen and Nicholls (1999) showed that the constant speed rotary motion is probably the primary factor in creating shapes that were nearly round and in keeping the instrument centered in the canal during shaping 7.
Also less preflaring seems necessary with the Ni-Ti rotary systems as compared to hand filing. This can result in more conservative preparation, leaving more of the dentine intact and thus reducing the chances of transportation and maintaining better centering ability. This result of this investigation confirms other studies on comparison between hand and rotary Ni-Ti systems. Glosson et al. (1995) in their study found rotary Ni-Ti instruments to stay better centered in the canal as compared to hand Ni-Ti instruments 4. The apical 4 mm section in both groups showed greatest transportation and the coronal 12 mm section the lowest. Schafer et al. (2003) conducted their study on the relationship between taper size and flexibility and concluded that Ni-Ti files with taper greater than 0.04 should not be used for apical preparations of curved canals 8.
Conclusion
The canal preparation in natural teeth with rotary ProTaper files and hand ProTaper files revealed better results with rotary ProTaper files in terms of both factors evaluated. Rotary ProTaper files cause less transportation and remained better centered in the canal than hand ProTaper files.
References
1. Civjan S, Huget EF, DeSimon LB. Potential applications of certain nickel-titanium (Nitinol) alloys. J Dent Res. 1975;54(1):89-96. [ Links ]
2. Gambill JM, Alder M, Del Rio CE. Comparison of Ni-Ti and Stainless steel hand-file instrumentation using computed tomography. J Endod. 1996;22:369-75.
3. Garip Y, Gunday M. The use of computed tomography when comparing nickel-titanium and stainless steel files during preparation of simulated curved canals. Int Endod J. 2001;34(6):452-7.
4. Glosson CR, Haller RH, Dove SB, Del Rio CE. A comparison of root canal preparations using Ni-Ti hand, Ni-Ti engine-driven, and K-Flex endodontic instruments. J Endod. 1995;21(3):146-51.
5. Hartmann MS, Barletta FB, Camargo Fontanella VR, Vanni JR. Canal transportation after root canal instrumentation: a comparative study with computed tomography. J Endod. 2007;33(8):962-5.
6. Morgan L, Montgomery S. An evaluation of the crown-down pressureless technique. J Endod. 1984;10:491-8.
7. Ottosen SR, Nicholls JI. A comparison of instrumentation using naviflex and profile Ni-Ti engine-driven rotary instruments. J Endod. 1999;25(6):457-60.
8. Schafer E, Schulz-Bongert U, Tulus G. Comparison of hand stainless steel and Ni-Ti rotary instrumentation: a clinical study. J Endod. 2003;30(6):432-5.
9. Schneider SW. A comparison of canal preparation in straight and curved root canals. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1971;32:271-5.
10. Tademir T, Aydemir H, Inan U, Unal O. Comparison with Hero 642 rotary Ni-Ti instruments compared with stainless steel hand K-file assessed using computed tomography. Int Endod J. 2005;38:402-8.
11. Usman N, Baumgartner JC, Marshall JG. Influence of instrument size on root canal debridement. J Endod. 2004;30:110-2.
12. Walia H, Brantley WA, Gerstein H. An initial investigation of the bending and torsional properties of nitinol root canal files. J Endod.1988;14:346-51.
 Correspondence:
Correspondence:
Amit Gandhi
57-L Model Town, Rohtak-124001
Haryana – India
E-mail: amitgandhi2008@rediffmail.com
Received for publication: March 14, 2011
Accepted for publication: April 13, 2011
