










Services on Demand
Article
 pdf in English
pdf in English Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailRelated links
Share

 Permalink
PermalinkRSBO (Online)
On-line version ISSN 1984-5685
RSBO (Online) vol.9 n.3 Joinville Jul./Sep. 2012
Original Research Article
Avulsion of permanent teeth with open apex: a systematic review of the literature
Felipe G. Belladonna I ; Ane Poly I ; João M. S. Teixeira I ; Viviane D. M. A. Nascimento I; Sandra R. Fidel I ; Rivail A. S. Fidel I
ABSTRACT
Introduction: Considered the most serious of dental injuries, avulsion is known as the total displacement of tooth out of its socket. Treatment includes immediate replantation and its success is directly related to several factors. Objective: This paper aimed to review the literature in a systematic way on dental avulsion of permanent teeth with open apex, covering various topics such as: reason for avulsion; storage media; time out of the socket; use of antibiotics; splinting time; tooth vitality; presence of resorption and/or obliteration of pulp canal; and following-up time. Material and methods: PubMed/MedLine database and Dental Traumatology journal were searched, from May to June of 2011, and several studies comprising the current and classic literature were listed using the following terms: tooth avulsion, open apex, permanent and case report. Results and conclusion: Twelve cases reports were selected. Cases of dental trauma in open apex teeth may have a good prognosis if the following steps are taken: the hydration of the tooth and immediately replantation. It is important to search dental care, even if everything seems solved, and the tooth following-up should be performed periodically as informed by the dentist.
Keywords: tooth avulsion; tooth replantation; tooth injuries.
Introduction
During the last decades tooth trauma has been considered an increasing problem of public health, unlike dental caries which is in decreasing for years 22,28,33. The prevalence of traumatized teeth reported by literature varies from 10 to 51%. It is known that tooth trauma may have not only physical but also economical, social and psychological severe consequences 13.
Among all tooth lesions, avulsion is the most serious one 16. It is characterized by the complete displacement of the tooth out of its socket, severely affecting the pulp, periodontal ligament and alveolar bone 8,42. The frequency of avulsion in permanent dentition is from 0.5 to 16% 19,35. The avulsion lesions in children occur more frequently from 7 to 9 years-old 31, when the permanent incisors are erupting, most in boys than girls 41. In most of the times, the lesion involves a single tooth only, and maxillary central incisor is the most avulsed teeth 9.
Immediate replantation is the treatment of choice for the cases of tooth avulsion 19. However, because of several factors as lack of knowledge on what to do at the moment of the accident, this rarely occurs 5,30. When the tooth is not replanted at the moment of its avulsion, the patient should be guided to keep it in an appropriate medium and search for a dentist 35. According to Trope 39, this storage aims to decrease the post-replantation inflammatory response, avoiding the tooth dryness and maintaining the viability of the periodontal ligament cells.
The result of tooth avulsion treatment, as well as the occurrence of post-traumatic complications in the future, does not only depend on the time interval between the accident and the dental treatment – which ideally should be performed from 20 to 30 minutes –, but also on the medium in which the avulsed tooth was kept until the dentist appointment 8,40.
The aim of this study was to evaluate, through a systematic literature review, the main clinical and radiographic characteristics of cases reports on the avulsion of permanent tooth with open apex, such as: reason for avulsion; storage of the tooth; time out of tooth socket; use of antibiotics; time of splinting; tooth vitality; presence of resorption and/or root canal obliteration; and following-up period.
Methodology
To perform this literature review, the studies were searched either through PubMed/MedLine database or directly in Dental Traumatology journal. At the same time, a cross search was carried out, considering the bibliographic references of the papers selected. On PubMed/MedLine database, the following terms were employed: avulsion AND open apex (23); avulsion AND open apex AND permanent (14). Following, considering the time interval from June of 2006 and June of 2011, a new search was performed with the following terms: avulsion AND tooth AND case report (180). Considering the Dental Traumatology journal, the papers on avulsion (29), at the aforementioned time interval, were searched among the total of 567 papers published in that period.
The search was performed from May to June of 2011 by all authors, which also evaluated the results together. Firstly, the selection of the papers was executed based on their abstracts; following, the complete texts were analyzed. Inclusion criteria comprised studies published from June of 2006 to June of 2011, on the clinical and radiographic findings of the avulsion of permanent tooth with open apex. Exclusion criteria comprised: a) studies on animals or laboratorial studies; b) studies on primary teeth; c) literature reviews; d) intentional extractions, transplants and luxations. Editorials, summaries, and studies inaccessible through available databases or libraries were also excluded.
Results
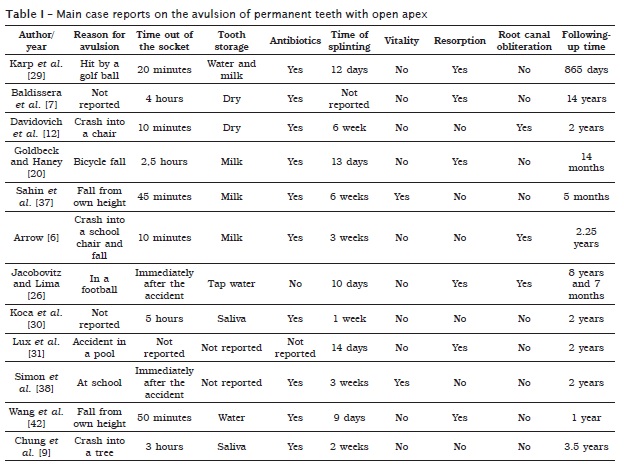
After the reading of the abstracts, the elimination of duplicate studies and evaluation according to inclusion and exclusion criteria, the first and second searches on PubMed/MedLine database resulted in 7 and 14 case reports, respectively; and 3 case reports in Dental Traumatology journal. After the complete reading of the papers selected, 12 case reports were included (table I).
A research conducted in Brazil 22 concluded that the avulsion was the most common type of trauma, affecting 32.9% of the teeth; 29.4% of the cases occurred in primary dentition and in 34% in permanent dentitions.
Immediate replant of an avulsed tooth is the ideal emergency procedure of choice to be performed at the accident site, as observed by Rai et al. 36. In that study, the authors reported a case of a 15-year-old boy who searched for treatment because of a purulent infection in the area of a tooth replanted by him six years ago. The endodontic treatment was performed and after 4 years of radiographic following-up, the lesion disappeared and there were no signals of resorption
The great concern is that most of population does not have such knowledge and generally is referred to medical emergency after the accident. A research 1 conducted with doctors and dentists concluded that 83.3% of the doctors do not have any knowledge on how to proceed in cases of traumatized teeth, while 93.3% of the dentists showed the required knowledge.
Discussion
Among all face lesions, tooth trauma is the most common one, from which tooth avulsion occurs in 0.5 to 16% of these cases 1,9. A comparison among the prevalence of trauma lesions in several countries for primary and permanent dentition showed that boys are affected at a double frequency of that of girls 41, with peaks of incidence from 7 to 9 years, when the permanent central incisors are erupting and the periodontal ligament shows only a minimum resistance to the extrusive force 15,31,40. Tooth trauma was prevalent in primary dentition (at 5 years-old) in 31 to 40% of boys and in 16 to 30% of girls. In permanent dentition (at 12 years-old), the prevalence ranges from 12 to 33% in boys and from 4 to 19% in girls 3.
Frujeri and Costa Jr. 18 reported in a research conducted in Brazil that the fall (20%) was the most common cause of tooth trauma, followed by accidents occurred during sports practice (10%), physical aggression (9%), car accidents (6%) and fights (4%). Other factors (2%), such as fainting and work accidents were also cited. By analyzing the main case reports searched by this systematic literature review, it was observed that the most frequent causes of avulsion were related to falls and to accidents due to sports practice.
Tooth replant success directly depends on the period of extra-alveolar time and on the storage medium used to keep the tooth up to replantation 2,5.
Cvek et al. 11 demonstrated that 13% of the teeth kept dry for 15 minutes, 40% kept dry from 20 to 40 minutes and 100% kept dry for more than 60 minutes showed signals of ankylosis. Therefore, the prevention of the periodontal ligament drying is of extreme importance. The extra-oral dry time results in irreversible damage to the periodontal ligament cells, which after replantation provokes a inflammatory response in a diffuse area of the root surface, leading to ankylosis and consequently to tooth loss. Excepting Baldissera et al. 7, Goldbeck and Haney 20, Koca et al. 30, Chung et al. 9, who replanted the tooth after a period longer than 60 minutes, and Lux et al. 31 who did not report the time amount in which the tooth was kept out of its socket, all other cases were replanted in less than 60 minutes.
The best treatment choice for an avulsed tooth is immediate replantation, so that the damages to the periodontal ligament cells are decreased and the ideal healing without resorption is achieved. Notwithstanding, this rarely occurs, because of factors such as the emotional stress of the people involved and the lack of knowledge on first aid 30. When immediate replantation is not performed, the tooth should be kept in humid conditions. There are solutions capable of preserving the viability of the periodontal ligament cells for the time amount that these cells are out of the tooth socket. The main solutions are: water, which although protecting the tooth from dehydration (because it is a hypotonic medium) it provokes the fast lysis of the periodontal ligament cells; saliva, which has small osmolarity, contributing for the increasing of the harmful effects of bacterial contamination and presents as the only advantage the fact of being easily available; saline solution, which shows compatible osmolarity with the periodontal ligament cells, but lacks of nutrients such as calcium, magnesium and glucose required for a normal functioning of the metabolism of these cells; milk, which the medium indicated for the American Association of Endodontics as the solution for avulsed teeth because it maintains the viability of the periodontal ligament cells and it is significantly better than the other solutions because of its physiological properties, including pH and osmolarity compatible with that of the periodontal ligament cells, although it is not capable of revitalizing degenerated cells; and Hank`s balanced salt solution, which is considered the best storage medium for avulsed teeth because it has ideal osmolarity and pH and it is very efficient for the preservation and even regeneration of the periodontal ligament cells 14,21. In the papers researched by this literature review, most of the case reports used milk as storage medium. For the studies of Jacobovitz and Lima 26 and Simon et al. 38, the tooth was replanted immediately after the avulsion.
Teeth with incomplete apexes which are replanted in less than 60 minutes after the avulsion may recover because of pulp revascularization. However, this healing process did not occur in several times because the apical tissue is highly susceptible to bacterial contamination 17. Cvek et al. 10 reported that in teeth with open apexes, to avoid the contamination of the root surface could promote pulp revascularization. For this purpose, Wang et al. 42 recommended to immerse the avulsed tooth in doxycycline for 5 minutes prior to the replantation. After the replantation, tetanus prophylaxis and systemic antibiotics should also be prescribed for the patient 2. All studied included in this literature review used systemic antibiotics after replantation, except for the studies of Jacobovitz and Lima 26 and Lux et al. 31.
Currently, semi-rigid splinting is used to help the periodontal healing. The current protocols recommend the splinting for teeth undergoing luxation, avulsion or root fracture. Studies indicated that the splinting type and time were not significant variables when related to the healing outcomes 27,34.
According to Hinckfuss and Messer 25, the success probability of periodontal healing after replantation is not affected by the splinting time. The vitality of periodontal ligament cells strongly affected by the extra-oral time amount and the storage conditions may have a higher effect on the splinting period. Basically, three tissues are involved in the healing after tooth replantation: the pulp, periodontal ligament and alveolar bone. After trauma, the pulp may present three healing modalities: survival, obliteration or necrosis. This latter has a fundamental role in the post-traumatic development of external root resorption 8.
A study based on evidences of 236 permanent teeth replanted after avulsion concluded that the probability of well-successful periodontal healing was improved by extirpating the pulp in a period of 14 days after replantation because it decreases the risk of developing inflammatory resorption 23. Additionally, according to Andreasen and Andreasen 3, a tooth referred to replantation must not show advanced periodontal disease and the alveolar socket must be reasonably intact; also, extraoral periods exceeding 1 hour are generally associated with root resorption. Corroborating this idea, all case reports in which the tooth was replanted in less than 1 hour did not show resorption signals, except in the study of Karp et al. 29.
The tooth may be in function for 20 years or more after its replantation 32. Additionally, the closer to the rizogenesis ending, the higher will be its longevity 4. In replanted teeth, frequently ankylosis may develop in sites of inflammatory resorption previously stopped.
According to the Guidelines on avulsion published by Flores et al. 17, the proper treatment of different cases of avulsion is described below. In cases of teeth with open apex, replanted before searching for treatment, the site must be cleaned by air jets, saline or chlorhexidine; the extraction of the tooth is not indicated. If the patient comes to treatment with the tooth out of the socket, root surface and apical foramen must be cleaned by saline, as well as the socket for removing blood clot; next, the socket should be examined which must be repositioned in cases of fracture, and finally, the tooth must be replanted by gentle digital pressure. In these cases, semi-rigid splinting must be maintained for up to 2 weeks. However, if the tooth was kept in extraoral time longer than 60 minutes, the prognosis would not be favorable. The goal of performing such replantation is to promote alveolar bone growth to encapsulate the replanted tooth. The expected result is an eventual ankylosis and root resorption. The proper procedure is to remove the necrotic tissue gently with the aid of gauze. Root canal treatment may be performed either prior to replantation or 7 to 10 days after it, although in cases of open apex endodontic treatment should be performed prior to replantation. Following, it is necessary to immerse the tooth in a 2% sodium fluoride solution for 20 minutes and then performing its replantation. In this case, the semi-rigid splinting should be kept for until 4 weeks. From that moment on, the treatment is the same for all cases: to suture possible lacerations; verify clinical and radiographically the normal position of the replanted tooth; apply a semi-rigid splinting and administrate systemic antibiotics; if the avulsed tooth was in contact with the ground, tetanus vaccine must be prescribed; start the endodontic treatment 7 to 10 days after replantation, by employing calcium hydroxide as intracanal medication for until one month followed by root canal obturation. This must be executed prior to the splinting removal. Next, the tooth must be followed-up. In teeth with open apex, such treatment should be avoided unless there should be clinical and radiographic evidence of pulp necrosis. The patient must follow a soft diet for until two weeks, perform oral hygiene with soft-bristle toothbrush after every meal and rinse with 0.1% chlorhexidine solution twice a day for one week.
The replanted teeth should be followed-up frequently during the first year (once a week in the 1st month, then once a month at the 3rd, 6th and 12th month) and, then, annually. The clinical and radiographic examinations will provide information to determine the result of the replantation procedure. The result is considered positive when the tooth is asymptomatic, with normal mobility and normal sound to percussion, in addition to the radiographic evidence of the continuation of root formation and obliteration of root canal, which is considered a rule. On the other hand, the result is considered negative when the tooth is symptomatic with either excessive or no mobility (ankylosis) and showing a metallic sound to percussion. In ankylosis cases, tooth crown seemed to be in infraocclusion. Additionally, the radiographic evidence of resorption (inflammatory, related to infection; or substitutive, related to ankylosis) is seen as a negative result 17.
Other critical question on tooth trauma outcomes is the patients compliance to treatment. In many cases, the patient must return to appointments many times, either for only clinical and radiographically examinations or for uncomfortable procedures. This is the most common cause of treatment drop-out by the patients 15.
Conclusion
The most frequent causes of tooth avulsion in teeth with open apex are related to falls and accidents in sports practice. The immediate replantation is considered the best treatment choice. If this is not possible, the tooth should be kept in an appropriate medium and the patient should seek the dentist urgently. On the other hand, the dentist must be prepared and updated to follow a relevant protocol in each case, guiding the patient on the importance of the following-up appointments. The healing process should be followed-up for a long period, therefore enabling an early treatment at the first signs of pulp necrosis and/or root resorption.
References
1. Abu-Dawoud M, Al-Enezi B, Andersson L. Knowledge of emergency management of avulsed teeth among young physicians and dentists. Dent Traumatol. 2007;23:248-55. [ Links ]
2. Andreasen JO, Andreasen FM, Andersson L. Textbook and color atlas of traumatic injuries to the teeth. 4. ed. Copenhagen: Munksgaard; 2007. p. 479-80.
3. Andreasen JO, Andreasen FM. Texto e atlas colorido de traumatismo dental. 3. ed. Porto Alegre: Artmed; 2001. p. 399.
4. Andreasen JO, Borum MK, Andreasen FM. Replantation of 400 avulsed permanent incisors. III. Factors related to root growth after replantation. Endod Dent Traumatol. 1993;11:69-75.
5. Andreasen JO, Borum MK, Jacobsen HL, Andreasen FM. Replantation of 400 avulsed permanent incisors II. Factor related to periodontal ligament healing. Endod Dent Traumatol. 1995;11:76-89.
6. Arrow P. An unusual healing of a replanted permanent lateral incisor. Aust Dent J. 2009;54:57-60.
7. Baldissera EZ, Fontanella VR, Ito W, Pomar F. Use of hydroxy-apatite in tooth replantation radiographically followed up for 14 years: a case report. Dent Traumatol. 2007;23:47-50.
8. Chappuis V, Von Arx T. Replantation of 45 avulsed permanent teeth: a 1 year follow-up study. Dent Traumatol. 2005;21:289-96.
9. Chung H, Kim M, Yang W, Ko H. An interesting healing outcome of a replanted immature permanent tooth: a case report. Dent Traumatol. 2011;27:77-80.
10. Cvek M, Cleaton-Jones P, Austin J, Lownie J, Kling M, Fatti P. Effect of topical application doxycycline on pulp revascularization and periodontal healing in reimplanted monkey incisors. Endod Dent Traumatol. 1990;6:170-7.
11. Cvek M, Granath LE, Hollender L. Treatment of non-vital permanent incisors with calcium hydroxide. Part 3. Variation of occurrence of ankylosis of reimplanted teeth with duration of extra-alveolar period and storage environment. Odontol Revy. 1974;25(1):43-56.
12. Davidovich E, Moskovitz M, Moshonov J. Replantation of an immature permanent central incisor following pre-eruptive traumatic avulsion. Dent Traumatol. 2008;24:e47-52.
13. Emerich K, Czerwinska M, Ordynied-Kwasnica I. Immediate self-replantation of an avulsed permanent mandibular incisor – a case report. Dent Traumatol. 2010;26:443-6.
14. Ferreira EL, Filho FB, Correr GM, Leonardi DP, Fariniuk LP, Campos EA et al. Dental avulsion, from dental replantation to dental implant: a case report with a 20-year follow up. Braz J Dent Traumatol. 2009;1(1):13-9.
15. Fidel SR, Santiago MRJ, Reis C, Pinho MAB, Fidel RAS. Successful treatment of a multiple dental trauma: case report of combined avulsion and intrusion. Braz J Dent Traumatol. 2009;1(1):32-7.
16. Flores MT, Andersson L, Andreasen JO, Bakland LK, Malmgren B, Barnett F et al. Guidelines for the management of traumatic dental injuries. I. Avulsion of permanent teeth. Dent Traumatol. 2007;23:66-71.
17. Flores MT, Andersson L, Andreasen JO, Bakland LK, Malmgren B, Barnett F et al. Guidelines for the management of traumatic dental injuries. II. Avulsion of permanent teeth. Dent Traumatol. 2007;23:130-6.
18. Frujeri MLV, Costa Jr EDC. Effect of a single dental health education on the management of permanent avulsed teeth by different groups of professionals. Dent Traumatol. 2009;25:262-71.
19. Fridstrom M, Schollin J, Crossner CG. Evaluating Emdogain and healing of replanted teeth using an intra-individual experimental-control study design. Dent Traumatol. 2008;24:299-304.
20. Goldbeck AP, Haney KL. Replantation of an avulsed permanent maxillary incisor with an immature apex: report of a case. Dent Traumatol. 2008;24:120-3.
21. Gomes MCB, Westphalen VPD, Westphalen FH, Neto UXS, Fariniuk LF, Carneiro E. Study of storage media for avulsed teeth. Braz J Dent Traumatol. 2009;1(2):69-76.
22. Gulinelli JL, Saito CTMH, Garcia-Júnior IR, Panzarini SR, Poi WR, Sonoda CK et al. Occurrence of tooth injuries in patients treated in hospital environment in the region of Araçatuba, Brazil during a 6-year period. Dent Traumatol. 2008;24:640-4.
23. Hinckfuss SE, Messer LB. An evidence-based assessment of the clinical guidelines for replanted avulsed teeth. Part I: timing of pulp extirpation. Dent Traumatol. 2009;25:32-42.
24. Hinckfuss SE, Messer LB. An evidence-based assessment of the clinical guidelines for replanted avulsed teeth. Part II: prescription of systemic antibiotics. Dent Traumatol. 2009;25:158-64.
25. Hinckfuss SE, Messer LB. Splinting duration and periodontal outcomes for replanted avulsed teeth: a systematic review. Dent Traumatol. 2009;25:150-7.
26. Jacobovitz M, Lima RKP. The use of calcium hydroxide and mineral trioxide aggregate on apexification of a replanted tooth: a case report. Dent Traumatol. 2009;25:e32-6.
27. Kahler B, Heithersay GS. An evidence-based appraisal of splinting luxated, avulsed and root-fractured teeth. Dent Traumatol. 2008;24:2-10.
28. Kargul B, Welbury R. An audit of the time to initial treatment in avulsion injuries. Dent Traumatol. 2009;25:123-5.
29. Karp J, Bryk J, Menke E, McTigue D. The complete endodontic obturation of an avulsed immature permanent incisor with mineral trioxide aggregate: a case report. Pediatr Dent. 2006;28:273-8.
30. Koca H, Topaloglu-Ak A, Sütekin E, Koca O, Acar S. Delayed replantation of an avulsed tooth after 5 hours of storage in saliva: a case report. Dent Traumatol. 2010;26:370-3.
31. Lux H, Goetz F, Hellwig E. Case report: endodontic and surgical treatment of an upper central incisor with external root resorption and radicular cyst following a traumatic tooth avulsion. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010;110:e61-7.
32. Mackie IC, Worthington HV. An investigation of replantation of traumatically avulsed permanent incisor teeth. Br Dent J. 1992;172:17-20.
33. Manfrin TM, Boaventura RS, Poi WR, Panzarini SR, Sonoda CK, Sundefeld MLMM. Analysis of procedures used in tooth avulsion by 100 dental surgeons. Dent Traumatol. 2007;23:203-10.
34. Moule AJ, Moule CA. The endodontic management of traumatized permanent anterior teeth: a review. Aust Dent J. 2007;52(1 Suppl):S122-37.
35. Qazi SR, Nasir KS. First-aid knowledge about tooth avulsion among dentists, doctors and lay people. Dent Traumatol. 2009;25:295-9.
36. Rai P, Gupta U, Kalra N. Self-replantation of an avulsed tooth in torsoversion: a 10-year follow-up. Dent Traumatol. 2007;23:158-61.
37. Sahin S, Saygun NI, Kaya Y, Ozdemir A. Treatment of complex dentoalveolar injury – avulsion and loss of periodontal tissue: a case report. Dent Traumatol. 2008;24:581-4.
38. Simon S, Lumley PJ, Cooper PR, Berdal A, Machtou P, Smith AJ. Trauma and dentinogenesis: a case report. J Endod. 2010;36:342-4.
39. Trope M. Clinical management of the avulsed tooth: present strategies and future directions. Dent Traumatol. 2002;18:1-11.
40. Tzigkounakis V, Merglová V, Hecová H, Netolicky J. Retrospective clinical study of 90 avulsed permanent teeth in 58 children. Dent Traumatol. 2008;24:598-602.
41. Vasconcellos LGO, Brentel AS, Vanderlei AD, De Vasconcellos LMR, Valera MC, De Araújo MAM. Knowledge of general dentists in the current guidelines for emergency treatment of avulsed teeth and dental trauma prevention. Dent Traumatol. 2009;25:578-83.
42. Wang SH, Chung MP, Su WS, Cheng JC, Shieh YS. Continued root formation after replantation and root canal treatment in an avulsed immature permanent tooth: a case report. Dent Traumatol. 2010;26:182-5.
 Correspondence:
Correspondence:
Felipe G. Belladonna
Rua Otávio Carneiro, 64 – ap. 703
CEP 24230-191 – Icaraí – Niterói – Brasil
E-mail:felipebelladonna@hotmail.com
Received for publication: August 09, 2011.
Accepted for publication: January 09, 2012.
