










Services on Demand
Article
 pdf in English
pdf in English Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailRelated links
Share

 Permalink
PermalinkRSBO (Online)
On-line version ISSN 1984-5685
RSBO (Online) vol.9 n.3 Joinville Jul./Sep. 2012
Literature Review Article
Comprehensive review of caries assessment systems developed over the last decade
Abhishek Mehta I
ABSTRACT
Introduction:World Health Organization (WHO) in the year 2007 recognized the growing burden of oral diseases worldwide and emphasized the need to scale up action based on comprehensive data collection systems. In view of the global epidemic of untreated caries in children there is an urgent need to establish a scoring system that both assesses and quantifies various advanced stages of caries. Furthermore, the available data are not readily comparable due to the different scoring systems used. The DMF index despite having limitations has been widely utilized in oral epidemiological surveys. It is recommended by the WHO for measuring and comparing the experience of dental caries in populations. The path of future research in caries epidemiology will depend on finding an ideal caries index. Objective:This review is prepared to present and critically evaluate various new caries assessment systems that have been developed in the last decade. Literature review: A literature search was done to find out major caries assessment systems developed over last decade, it revealed there were five new indices developed to assess caries. These indices were critically evaluated to list their strengths and limitations. Conclusion:There are many promising new caries indices purposed, but still there is a need for further studies to evaluate their validity and reliability before they can replace DMFT index.
Keywords: caries assessment; DMF index; significant caries index; ICDAS; specific caries index; PUFA; CAST.
Introduction
Dental caries is a complex disease affecting the teeth, which is mainly caused by imbalance between demineralization and remineralization process around the tooth surface. It is a major cause of tooth loss and pain around the world. Caries incidence is witnessing a decline in developed countries due to proper availability of fluoride products, better oral health services and awareness regarding etiology of caries. At the same time incidence of caries is increasing in developing countries 13. Research over the years has shown that caries is a preventable and controllable disease. To apply measures which can prevent or control caries, a reliable picture of it in a population is prerequisite; this can only be obtained if we have a reliable caries assessment system (index).
For several decades dental researchers are following and teaching DMF index developed by Klein, Palmer and Knutson in 1938 for assessing dental caries 11. World health organization has adopted this index in its oral health assessment form for conducting national oral health surveys 16. Various reasons can be stated for its continued use for assessing caries, foremost of them are: it is simple to use, valid and reliable, that is why it is still being used for assessment and comparison of caries status of the population groups around the world. However DMF index is facing criticism on various points (table I).
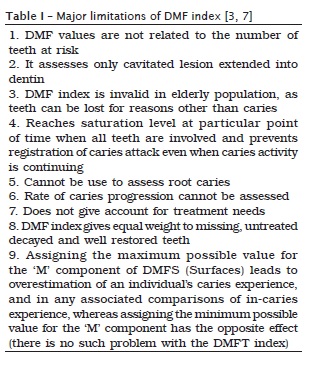
From the public health viewpoint, major disadvantage of using DMF index is that it records only cavitated lesions and ignore incipient carious lesions. These lesions can be reversed by application of various preventive measures like fluorides if detected at earlier stages. So an index should be able to record these lesions to apply primary preventive measures in a population. The objective of this literature review is to critically evaluate major caries assessment systems purposed in last one decade and try to build up requisites for an ideal caries index.
Significant Caries (SiC) Index
Brathall 2 introduced this index in order to bring attention to the individuals with the highest caries values in each population under investigation. It tries to overcome limitation of the mean DMFT value in accurately assessing the skewed distribution of dental caries in a population especially in developed countries leading to incorrect conclusion that the caries situation for the whole population is controlled, while in reality, several individuals still have caries. This problem was analysed in detail in a study conducted in Nevada which confirmed that dental caries remains a common chronic disease among Nevada youth, and the mean SiC score was significantly higher than DMFT scores within each survey year across comparison groups (p < 0.001). The authors concluded that using both caries indices (DMF and SiC) together may help to highlight oral health inequalities more accurately among different population groups within the community in order to identify the need for special preventive oral health interventions 5.
SiC is calculated by sorting individuals according to their DMFT values, than one third of the population with the highest caries scores is selected and the mean DMFT for this subgroup is calculated. This value is the SiC Index. In this way investigators can bring to attention of authorities the need of preventive measures required for prevention/control of caries in this subgroup. Main disadvantage of SiC index is that this index is just an extension of DMF index as it follows same criteria for assessing dental caries and will have same limitations in assessing caries in a population as DMF index. Also this index is more of significance in population where caries prevalence is low and has a skewed distribution.
International Caries Detection and Assessment System (ICDAS) – I and II
ICDAS was developed in the year 2001 by the effort of large group of researchers, epidemiologists and restorative dentists 10. It is an attempt to find a common caries assessment system based on many available such systems. ICDAS was developed on the basis of insights gained from a systematic review of the literature on clinical caries detection systems 9. Use of the ICDAS was intended to make subsequent studies more useful for comparison, reviews or meta-analyses and thus fulfill the requirements of evidence-based dentistry 10,15. ICDAS-I was meant to include detection (D) of caries by stage of carious process, topography and anatomy, assessment (A) of caries process (whether cavitated or non-cavitated and active or arrested caries). But the ultimate index included detection of coronal caries and the assessment of lesion activity and root caries were not included due to lack of consensus and need for further discussions.
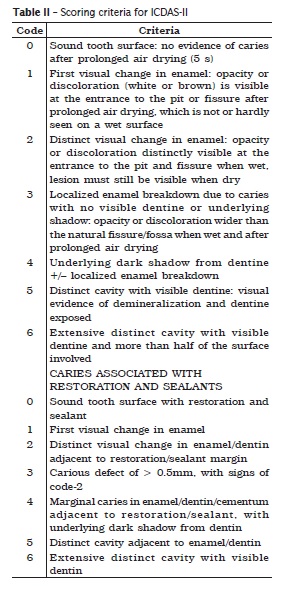
ICDAS coordinating committee came up with ICDAS-II in the year 2009 8 which describes both coronal caries and caries associated with restorations and sealants (CARS) (table II). Its codes for coronal caries ranges from 0 to 6, indicating the severity of the carious lesions involving pulp are not being scored. Details of scoring criteria can be accessed from the website of ICDAS (www.icdas.org). The advantages of the ICDAS-II are that it includes stages of carious lesion progression in the enamel and it has found to be a valid and reliable caries assessment system especially for clinical trials assessing effectiveness of caries preventive/ control agents 14. Shortcomings of ICDAS-II include: it is a complicated index due to the recording of non-primary caries lesion related conditions, does not correlate well with the detection and assessment of the conditions and various type of restorations and may lead to an overestimation of seriousness of dental caries experience 4.
Specific caries index
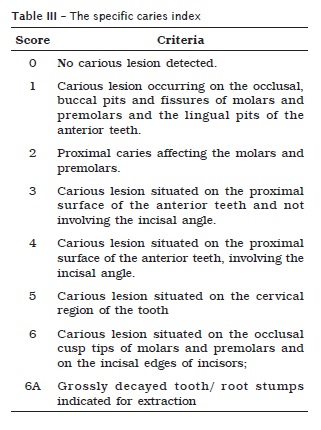
This index was purposed by Acharya 1 with the objective to develop a reproducible, surface specific caries index that would provide qualitative and quantitative information about untreated dental caries in an individual based on clinical examination and would provide, if used with DMFS index, useful data for planning oral health care for a target population. The scoring criteria of the index are shown in table below.
The index has shown good reliability and validity in the study conducted by original author but further search on various databases did not reveal any other study using this index 1. Some drawbacks of this index were - it employs same caries detection criteria as DMF or DMFS; in cases of large lesions, which cover more than one surface, only an assumption can be made regarding the originating lesion; the inability of this index, if used alone, to capture information useful for treatment planning; and the lack of provision for assessing root caries.
PUFA (pulp-ulcer-fistula-abscess) index
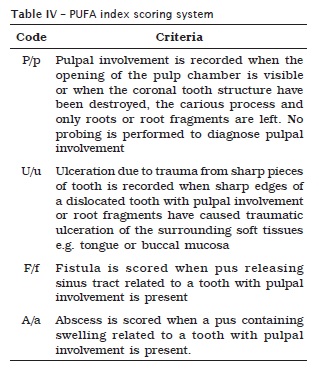
The failure of DMF index to provide information on the clinical consequences of untreated dental caries, such as pulpal abscess, which may be more serious than the carious lesions themselves, is the basis for the development of PUFA index 12. This index records the advanced stages of untreated caries lesions so that caries data collected should have impact on health decision makers, which is not possible with DMF index. Scoring method of PUFA index is described in table IV.
In many developing countries, access to oral health services is limited and teeth are often left untreated or are extracted because of pain or discomfort, such an index can provide useful information for researches and authorities. Strong points of this index can be simple to record, can be used for primary and permanent teeth and results can be presented alongside with DMF index. There are certain limitations appearing after a recent study 6 suggesting that there are few subjects with score u (ulcer) and assessment of abscess and fistula can be combined into one code. Hence reliability and validity of this index requires further discussion and research.
Caries assessment spectrum and treatment (CAST) index
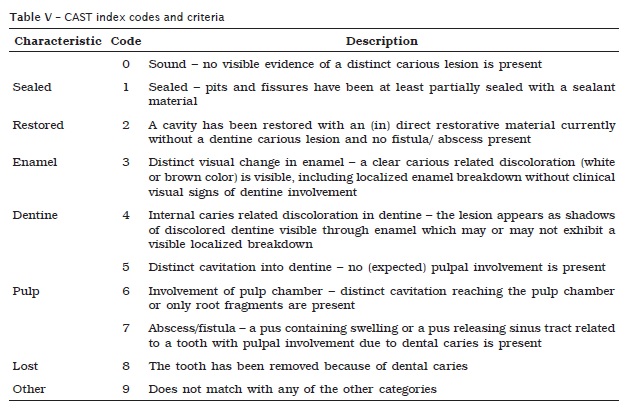
This index was developed because of the need to find a reliable, pragmatic cohesive and easy to read reporting system which is based on the strengths of PUFA and ICDAS-II indices and provide a link to the widely used DMF index (M and F component). It covers the total dental caries spectrum – from no carious lesion, through caries protection (sealant) and caries cure (restoration) to carious lesions in enamel and dentine, and the advanced stages of caries lesion progression in pulpal and tooth surrounding tissue (table V) 6. It does not record active and inactive carious lesions. The CAST index has not been validated, nor has its reliability been tested. It is also not suggested for use in clinical trials. Other limitation can be that it does not provide data on treatment or preventive measures required for each code.
Conclusion
This review found that while new caries detection criteria measured different stages of the caries process, there were inconsistencies on how the caries process was measured. The future of research, practice, and education in cariology requires the development of an integrated definition of dental caries and uniform systems for measuring the caries process. Many new indices have been developed to assess caries but we are far away from finding an ideal caries index which can replace or overcome limitations of DMF index. Some questions which remain unanswered in caries epidemiology are:
1. Is there a need to replace WHO recommended DMFT index especially for assessing caries in developing countries?
2. Should an ideal caries index suggest treatment needs of different caries stages?
3. What stage of the caries process should be measured; what are the definitions for each selected stage?
4. What is the best clinical approach to detect each caries stage on different tooth surfaces?
5. Should the research be separated with regard to find out an ideal coronal and root caries index?
6. Should separate indices be developed for assessing caries in oral health surveys and clinical trials? At last it is better to say in current scenario it will not be easy to replace DMF index as epidemiologists had collected or still collecting lot of data based upon this index.
References
1. Acharya S. Specific caries index: a new system for describing untreated dental caries experience in developing countries. J Public Health Dent. 2006;66(4):285-7. [ Links ]
2. Bratthall D. Introducing the Significant Caries Index together with a proposal for a new oral health goal for 12-year-olds. Int Dent J. 2000;50:378-84.
3. Broadbent JM, Thomson WM. For debate: problems with the DMF index pertinent to dental caries data analysis. Community Dent Oral Epidemiol. 2005;33:400-9.
4. De Amorin RG, Figueiredo MJ, Leal SC. Caries experience in a child population in a deprived area of Brazil, using ICDAS-II. Clin Oral Invest. 2011; DOI: 10.1007/s00784-011-0528-9.
5. Ditmyer M, Dounis G, Mobley C, Schwarz E. Inequalities of caries experience in Nevada youth expressed by DMFT index vs. Significant Caries Index (SiC) over time. BMC Oral Health. 2011;11:12-21.
6. Frencken JE, De Amorim RG, Faber J, Leal SC. The caries assessment spectrum and treatment (CAST) index rational and development. Int Dent J. 2011;61:117-23.
7. Hiremath SS. Indices. In: Hiremath SS. Textbook of preventive and community Dentistry. 2. ed. India: Elsevier; 2011. p. 198-221.
8. ICDAS Coordinating Committee (ICDAS CC). Rationale and evidence for the international caries detection and assessment system (ICDAS-II). 2005. Available from: URL: http://www.icdas.org.
9. Ismail AI. Visual and visuo-tactile detection of dental caries. J Dent Res. 2004;83:C56-66.
10. Ismail AI, Sohn W, Tellez M, Amaya A, Sen A, Hasson H et al. The International Caries Detection and Assessment System (ICDAS): an integrated system for measuring dental caries. Community Dent Oral Epidemiol. 2007;35:170-8.
11. Klein H, Palmer C. Studies on dental caries vs. familial resemblance in the caries experience of siblings. Pub Hlth Rep. 1938;53:1353-64.
12. Monse B, Heinrich-Weltzien R, Benzian H, Holmgren C, van Palenstein Helderman W. PUFA – An index of clinical consequences of untreated dental caries. Community Dent Oral Epidemiol. 2010;38:77-82.
13. Peterson PE. World Oral Health Report – 2003. Community Dent Oral Epidemiol. 2003;31 (Suppl. 1):3-24.
14. Pitts NB. How the detection, assessment, diagnosis and monitoring of caries integrate with personalized caries management. In: Pitts N (ed.). Detection, diagnosis and monitoring of caries. Basel: Karger; 2009. p. 1-14.
15. Richards D. Outcomes, what outcomes? (Editorial). Evid Based Dent. 2005;6:1.
16. World Health Organization. Oral health surveys – basic methods. 4. ed. Geneva: World Health Organization; 1997.
 Correspondence:
Correspondence:
Abhishek Mehta
Associate Professor and Head, Dept. of Public Health Dentistry
Dr. H. S. Judge Institute of Dental Sciences and Hospital, Panjab University Chandigarh (U.T.)
E-mail:mehta_abhishek2003@yahoo.co.in
Received for publication: November 25, 2011.
Accepted for publication: March 08, 2012.
