










Services on Demand
Article
 pdf in English
pdf in English Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailRelated links
Share

 Permalink
PermalinkRSBO (Online)
On-line version ISSN 1984-5685
RSBO (Online) vol.13 n.3 Joinville Jul./Sep. 2016
ORIGINAL RESEARCH ARTICLE
Health-related quality of life of patients undergoing rehabilitation with implant-supported prostheses
Monalisa KlingenfussI; Denise Piotto LeonardiI; Estela Maris LossoI; Tatiana Miranda DeliberadorI; Bárbara Pick OrnaghiI
I Master Program in Clinical Dentistry, Positivo University – Curitiba – Paraná – Brazil
ABSTRACT
Introduction: The success of oral reabilitation treatment depend on the re-establishment of the masticatory function and oral comfort of the patient. Objective: To evaluate the oral health-related quality of life (OHRQoL) of patients undergoing rehabilitation with implant-supported prostheses by Oral Health Impact Profile - short form questionnaire (OHIP-14) and a questionnaire associated to the Visual Analog Scale (VAS). Material and methods: Fourteen patients requiring implant-supported prostheses on anterior region were asked to complete the OHIP-14 before, 1 and 3 months, and the VAS questionnaire, 1 and 3 months after the prosthesis installation (sample group). Moreover, fourteen complete dentate patients were asked to complete the OHIP-14 (control group). For each OHIP-14 category, the sample group's answers were compared between the evaluation periods by the Kruskal-Wallis test, and to the control group's answers by the U-test. The answers of the questionnaire associated to VAS were compared between the evaluation periods by t-test (α=0.05). Results: For OHIP-14, there was no statistical difference between the answers after 1 and 3 months; however, there was difference among the answers of baseline, and 1 and 3 months after the prostheses installation, excepted for functional limitation. Comparing to the control group, before the prostheses installation, there was statistical difference for functional limitation, physical pain, psychological discomfort, physical and psychological disability; and, there was no difference after 3 months of prostheses installation. For the questionnaire associated to the VAS, there was no statistical difference between the responses for both evaluation periods, excepted for the prosthesis' comfort and stability. Conclusion: The rehabilitated patients showed a significant improvement in function, aesthetics, self-esteem, and the quality of life.
Keywords: dental implants; dental prosthesis; patient satisfaction.
Introduction
Longitudinal studies show that implantsupported prostheses (ISP) are a safe and predictable treatment method with high survival rates 10,13,16,17. Technically, the success of a dental restoration procedure can be defined as it can keep in position and it does not undergo any intervention throughout the whole period of observation 17. Nevertheless, this definition of success is usually set by the clinician or the researcher, not by the patient, the one who is interested the most in the final result of the treatment 2,8. Therefore, the success of oral reabilitation treatment should depend on the re-establishment of the masticatory function and oral comfort of the patient 1,21.
It was reported that the ISP problems are related to isolated aspects about restoration failures, instead of reporting on the functional survival rate of the prosthesis, which identifies the prosthetic functioning in the oral cavity, despite any fracture that can be repaired or a detachment in which the prosthesis can be re-cemented, and can be notice by the patient that will determine if the treatment achieve the success 17.
When a patient's expectations are not fulfilled by the treatment, typically psychosocial responses arise, such as anxiety, insecurity, lower self-esteem and introversion; which promote a negative effect on the patient's quality of life. Thus, the evaluation of prosthetic treatments with an approach centered more on patients' expectations is highly relevant 8. However, the capacity of dental clinicians and researchers to assess oral health have been hampered by limitations in measurements of the levels of dysfunction, discomfort, and disability associated with oral disorders. For this purpose the Oral Health Impact Profile 49 (OHIP-49) was developed which is a scaled index composed by forty nine unique statements describing the consequences of oral disorders on oral health-related quality of life (OHRQoL) 19. The short form of OHIP-49, called as OHIP-14, also measures the people's perceptions of the impact of oral conditions on their well-being 20. Nowadays, the use of validated questionnaires is a scientifically proven method to evaluate selfperception and improvement on the OHRQoL of patients rehabilitated with prostheses on implants 3,4,7,11.
Another method to evaluate OHRQoL is the use of the visual analog scale (VAS) associated to a questionnaire. Originally, VAS was developed to evaluate pain. Its advantages include easy application and understanding by patients, as well as the application of simple statistical tests to analyze the results. The aplicability of VAS for studies not related to pain evaluation had been proved 2,3,12,16.
The aim of this study was to evaluate the OHRQoL of patients undergoing rehabilitation with ISP on the anterior region, by means of OHIP-14 and a questionnaire associated with a VAS. The hypothesis tested in this study was that the patients after rehabilitation with ISP on the aesthetic region had a meaningful improvement in terms of functioning, aesthetics, ethics, self-esteem and, consequently, in their quality of life.
Material and methods
Experimental design
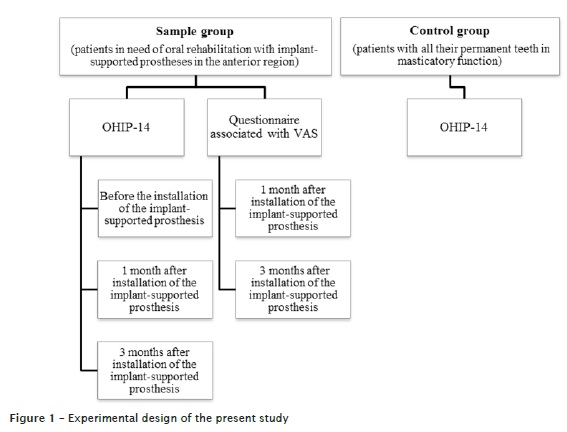
Fourteen patients of both genders, aged 20 to 85 years old, in need of oral rehabilitation with ISP on the anterior region were selected to compose the sample group. To compose the control group, fourteen patients of both genders, aged 20 to 85 years old, who had all their permanent teeth with masticatory function were selected.
For sample group, two questionnaires were applied: (i) OHIP-14, which was applied at baseline, 1 month, and 3 months after the installation of the ISP; and (ii) a questionnaire associated with VAS, which was applied 1 month and 3 months after the installation of the ISP. For control group, only the OHIP-14 was applied at one time (figure 1).
This study was approved by the Institutional Review Board regarding ethical aspects (protocol #54606). All patients signed an Informed Consent Form prior to the beginning of the study.
Implant-supported prostheses fabrication
All the patients of the sample group underwent the same ISP fabrication protocol, which started through reverse planning, implants installation, and the use of an immediate provisory removable partial prosthesis. None of patients received an immediate provisory implant-supported prosthesis.
Twelve patients received external hex prosthetic connection implants (Titamax TI, Neodent, Curitiba, Brazil) and two patients received Morse taper connection implants (Titamax CM EX, Neodent, Curitiba, Brazil). After 6 months of the implants installation, x-ray and clinical tests were performed to evaluate the osseointegration of the implants. Once no abnormalities were noticed, the healing abutments were placed on implants.
After seven days of the abutments installation, the impressions and transfers of the exact positions of the implants were done. For the external hex prosthetic connection implants, UCLA abutments were used; while for Morse taper connection implants, universal abutments were selected. After the proximal, occlusal and aesthetic adjustments of the prosthesis' ceramic, it was sent back to the laboratory for glaze coating. Finally, the prostheses on external hex prosthetic connection implants were screwed and the holes on top of the screws were blocked with gutta-percha (Tanari, Tanariman Indústria Ltda, Manacaru, Brazil) and composite resin (Charisma, Heraeus Kulzer, South Bend, USA). The prostheses on Morse taper connection implants were cemented with calcium hydroxide cement (Dycal, Dentsply, Rio de Janeiro, Brazil). After the final ISP installation, no occlusal or aesthetic adjustment was performed.
OHIP-14 Questionnaire
This questionnaire was designed to encompass seven theme categories: functional limitation, physical pain, psychological discomfort, physical, social and psychological disability, and handicap. Two questions were made for each category, totalizing 14 questions. The interview was made by a single interviewer, in the following way: the interviewer read out the questions and showed the patient the choices of objective answers numbered from 1 to 5 through a card, ranging from 1 = never, 2 = seldom, 3 = sometimes, 4 = frequently and 5 = always.
For each category, the means and the standard deviations of the answers to the corresponding questions were calculated. The data of each category were statistically compared within the evaluation periods (before the installation of the ISP, 1 month after and 3 months after the installation of the ISP) by means of the Kruskal-Wallis test. For multiple comparisons among means the Student-Newman- Keuls test was applied. Following that, the answers for each category of the sample groups in the evaluation periods baseline and 3 months after the installation of the prostheses were compared with the corresponding answers from the control group through the U of Wilcoxon-Mann-Whitney test for unpaired data. For all statistic analyses, the global significance level used was 5% (α = 0.05).
Questionnaire associated to VAS
To evaluate the level of satisfaction of the patient in relation to the implant-supported prosthesis a questionnaire associated to VAS was applied. This questionnaire was composed of questions related to the patient's general satisfaction in relation to the implant-supported prosthesis, the comfort and stability of the prosthesis, aesthetics, the patient's ability to perform oral hygiene, the patient's ability to speak wearing it, the patient's self-esteem, and its functioning. VAS ranges from zero to ten according to the patient's answers; zero means that the patient was completely dissatisfied while ten means that the patient was completely satisfied. Following a reading-out of the questions by a single interviewer, the patients marked the number of choices in the VAS.
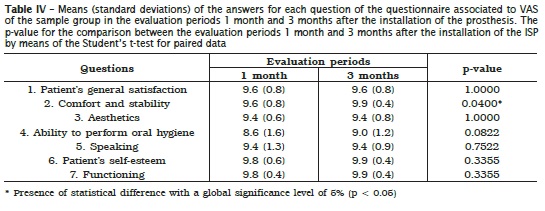
For each question the mean and the standard deviation of the answers from the patients were calculated. The data of each question were statistically compared between the evaluation periods 1 month and 3 months after the installation of the ISP by means of the Student's t-test for paired data (α = 0.05).
Results
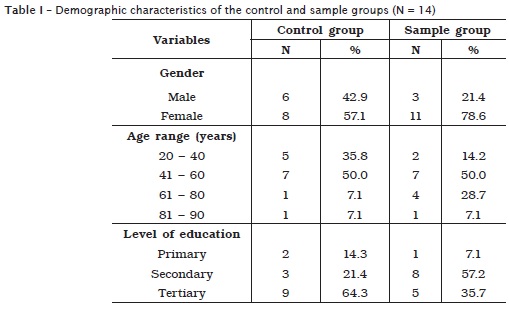
Table I shows the demographic characteristics of the sample and control groups, such as gender, age range, and level of education. Table II shows the means and the standard deviations of the answers for each category of OHIP-14 questionnaire of the sample group for the three evaluation periods, as well as the results of the Kruskal-Wallis analyses.
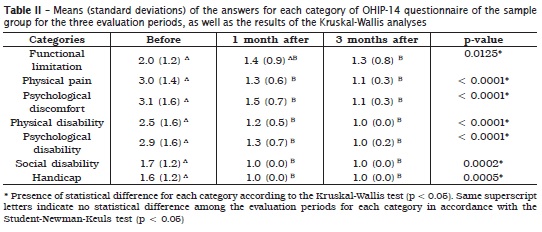
Based on those results, for all categories there was no statistical difference between the answers in the evaluation periods of 1 month and 3 months after the ISP installation. Nevertheless, there were statistical differences between the patients' answers referring to the period before the installation of the prostheses versus the answers referring to 1 and 3 months after the installation of the ISP. The only exception was the one referring to the functional limitation, which did not show any statistical difference.
Table III shows the means and the standard deviations for each category of OHIP-14 questionnaire of the control group, and the results of the statistical analyses when the answers to each category of the OHIP-14 questionnaire applied to the control group and the sample group before and 3 months after the installation of the ISP were compared. There was a significant statistical difference between the control and sample group answers before the installation of the prosthesis for the following categories: functional limitation, physical pain, psychological discomfort, physical disability, and psychological disability. However, when the control group answers were compared to the sample group answers for the period 3 months after the installation of the ISP there was no significant statistical difference between any of the categories in the OHIP-14 questionnaire. figure 2 shows the means of the answers for OHIP-14 questionnaire of the control group and the sample group for the three evaluation periods.
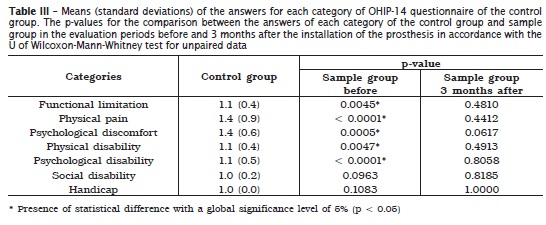
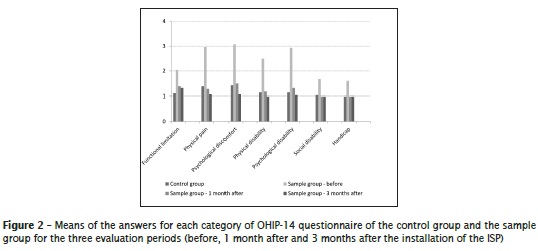
Table IV show the means, the standard deviations and the results of the statistical analyses when the patients' answers for the questionnaire associated to VAS in the periods 1 month and 3 months after the installation of the ISP were compared. Overall, there was no statistical difference between the answers referring to both evaluation periods, except for the question on comfort and stability, which showed a significant improvement of the patients' perception concerning this question. For both evaluation periods, the lowest mean obtained was that referring to the patient's ability to perform oral hygiene, but withotu statistical significant difference.
Discussion
The results of the present study seems to indicate that the OHRQoL of patients who underwent rehabilitation with ISP improved and could be comparable to the OHRQoL of patients who had all their permanent teeth with masticatory function. This is a statement that could only be made after the comparison of answers within the OHIP-14 questionnaire between the sample and the control groups. Thus, the control group established a parameter or a reference for the research variables 16.
The OHIP-14 questionnaire was considered a good indicator of the perceptions and feelings of patients about their own oral health and their expectations concerning the dental treatment 3,4,9,18. By comparing the answers of the sample group for the three evaluation periods, there was no statistical difference between the answers of 1 and 3 months after the installation of the prostheses for all categories. Probably there would be statistical difference between the answers if the evaluation had been done immediately after the installation of the ISP instead of one month after its installation. However, this type of comparison would have no clinical significance, because all types of dental prostheses requires an adaptation period. Recently, it was verified that the adaptation period for speaking among patients that received immediate protocol-type prostheses was 3 to 6 months 15. Considering the lower extension of the ISP in the present study, it is possible to realize that the adaptation period for our sample group patients was one month.
Nevertheless, there was statistical difference between the answers before and after the installation of the ISP. The only exception occurred for the functional limitation category, which did not present statistical difference between the periods before and 1 month after the installation of the prostheses. The functional limitation category is related to problems on pronouncing words and taste. So, this result shows that the re-establishment of speaking and taste probably requires more time for adaptation than the other characteristics, which is in accordance to previous studies 14,15.
The patients' satisfaction shown through answers of most OHIP-14's categories referring to 1 and 3 months after the ISP installation is justified by the fact that the patients were rehabilitated with temporary partial removable prostheses before the installation of the fixed ISP; which the former prosthesis type took a much larger intrabuccal area than the last one, causing discomfort to the patient. The same was found previously in which patients that received an implant overdenture were less satisfied and had lower OHRQoL than the patients who had a fixed ISP 4. This justification can also be used to explain the statistical difference found in most of the OHIP-14's categories when the answers of the control group and the sample group before the installation of the prostheses were compared (Table III).
After the comparison between the answers from the control group and those from the sample group 3 months after the installation of the ISP, no significant statistical difference was found among any of the categories in the OHIP-14 questionnaire, indicating similarity in OHRQoL between patients who had all their teeth performing masticatory function, and patients rehabilitated with ISP on the anterior region 3 months after installation. This type of improvement after prosthetic rehabilitation with implants had been also noticed 5-7,11,16,22. Based on these results, the hypothesis of this study was confirmed.
Considering the answers of the questionnaire associated to VAS from the sample group for both evaluation periods, there was no statistically significance differences, except for the question about comfort and stability, which showed a significant improvement in the mean perception of the patients to this matter. This result indicates that the improvement in comfort and stability may be attributed to the need for some time of adaptation for some patients after the rehabilitation with ISP, as previously reported 15. Moreover, the lowest mean obtained for the questionnaire associated to VAS was the facility to clean, despite not showing significant statistical differences. This result is explainable since the patients were firstly using partial removable prostheses, which could be removed for cleaning. The same was found in a previous study in which patients with ISP reported a greater difficulty with oral hygiene procedures than the controls with natural teeth 22.
Conclusion
Based on the answers to OHIP-14 and to the questionnaire associated to VAS obtained, the patients rehabilitated with implant-supported prosthesis on the anterior region reported a significant improvement in functioning, aesthetics, self-esteem, and consequently, in their OHRQoL.
References
1. Albrektsson T. Direct bone anchorage of dental implants. J Prosthet Dent. 1983 Aug;50(2):255-61. [ Links ]
2. Awad MA, Feine JS. Measuring patient satisfaction with mandibular prostheses. Community Dent Oral Epidemiol. 1998 Dec;26(6):400-5.
3. Borges TF, Mendes FA, Oliveira TRC, Gomes VL, Prado CJ, Neves F. Mandibular overdentures with immediate loading: satisfaction and quality of life. Int J Prosthodont. 2011;24(6):534-9.
4. Brennan M, Houston F, O'Sullivan M, O'Connell B. Patient satisfaction and oral health-related quality of life outcomes of implant overdentures and fixed complete dentures. Int J Oral Maxillofac Implants. 2010 Jul-Aug;25(4):791-800.
5. Bruyn H, Collaert B, Linden U, Bjorn AL. Patient's opinion and treatment outcome of fixed rehabilitation on Branemark implants. A 3-year follow-up study in private dental practices. Clin Oral Implants Res. 1997 Aug;8(4):265-71.
6. Cibirka RM, Razzoog M, Lang BR. Critical evaluation of patient responses to dental implant therapy. J Prosthet Dent. 1997 Dec;78(6):574- 81.
7. Erkapers M, Ekstrand K, Baer RA, Toljanic JA, Thor A. Patient satisfaction following dental implant treatment with immediate loading in the edentulous atrophic maxilla. Int J Oral Maxillofac Implants. 2011 Mar-Apr;26(2):356-64.
8 . Feine JS, Dufresne E, Boudrias P , Lund JP. Outcome assessment of implantsupported prostheses. J Prosthet Dent. 1998 May;79(5):575-9.
9. Furuyama C, Takaba M, Inukai M, Mulligan R, Igarashi Y, Baba K. Oral health-related quality of life in patients treated by implant-supported fixed dentures and removable partial dentures. Clin Oral Implants Res. 2012 Aug;23(8):958-62.
10. Gokcen-Rohlig B, Yaltirik M, Ozer S, Tuncer ED, Evlioglu G. Survival and success of ITI implants and prostheses: retrospective study of cases with 5-year follow-up. Eur J Dent. 2009 Jan;3(1):42-9.
11. Harle TJ, Anderson JD. Patient satisfaction with implant-supported prostheses. Int J Prosthodont. 1993 Mar-Apr;6(2):153-62.
12. Inoue M, John MT, Tsukasaki H, Furuyama C, Baba K. Denture quality has a minimal effect on health-related quality of life in patients with removable dentures. J Oral Rehabil. 2011 Nov;38(11):818-26.
13. Jung RE, Zembic A, Pjetursson BE, Zwahlen M, Thoma DS. Systematic review of the survival rate and the incidence of biological, technical, and aesthetic complications of single crowns on implants reported in longitudinal studies with a mean follow-up of 5 years. Clin Oral Implants Res. 2012 Oct;23(Suppl 6):2-21.
14. Levi A, Psoter WJ, Agar JR, Reisine ST, Taylor TD. Patient self-reported satisfaction with maxillary anterior dental implant treatment. Int J Oral Maxillofac Implants. 2003 Jan- Feb;18(1):113-20.
15. Molly L, Nackaerts O, Vandewiele K, Manders E, van Steenberghe D, Jacobs R. Speech adaptation after treatment of full edentulism through immediate-loaded implant protocols. Clin Oral Implants Res. 2008 Jan;19(1):86-90.
16. Pjetursson BE, Karoussis I, Burgin W, Bragger U, Lang NP. Patients' satisfaction following implant therapy. A 10-year prospective cohort study. Clin Oral Implants Res. 2005 Apr;16(2):185-93.
17. Pjetursson BE, Thoma D, Jung R, Zwahlen M, Zembic A. A systematic review of the survival and complication rates of implant-supported fixed dental prostheses (FDPs) after a mean observation period of at least 5 years. Clin Oral Implants Res. 2012 Oct;23(Suppl 6):22-38.
18. Ponsi J, Lahti S, Rissanen H, Oikarinen K. Change in subjective oral health after single dental implant treatment. Int J Oral Maxillofac Implants. 2011 May-Jun;26(3):571-7.
19. Slade GD. Derivation and validation of a shortform oral health impact profile. Community Dent Oral Epidemiol. 1997 Aug;25(4):284-90.
20. Slade GD, Spencer AJ. Development and evaluation of the oral health impact profile. Community Dent Health. 1994 Mar;11(1):3-11.
21. Wennerberg A, Albrektsson T. Current challenges in successful rehabilitation with oral implants. J Oral Rehabil. 2011 Apr;38(4):286-94.
22. Yi SW, Carlsson GE, Ericsson I, Kim CK. Patient evaluation of treatment with fixed implantsupported partial dentures. J Oral Rehabil. 2001 Nov;28(11):998-1002.
 Corresponding author:
Corresponding author:
Bárbara Pick Ornaghi
Rua Emiliano Perneta, 466, sala 605 – Centro
CEP 80420-080 – Curitiba – PR – Brasil
E-mail: ba@pick.com.br
Received for publication: April 12, 2016
Accepted for publication: July 4, 2016
